

Pulmonary bullae are defined as air spaces greater than 1cm in diameter with no epithelial wall. They can appear in normal pulmonary parenchyma, or more commonly, in the context of generalized emphysema. The natural course of pulmonary bullae is characterized by progressive growth, but it is not uncommon for them to present long periods of stability. In contrast, spontaneous regression is unusual.1
We report the case of a 55-year-old man, former smoker of 50 pack-years who gave up 16 years previously, who attended our hospital in June 2012 with cough, daily expectoration, and dyspnea MRC grade 1, with no significant exacerbations. Lung function tests showed a moderate obstructive pattern, with a forced vital capacity (FVC) of 4890cc (106%), forced expiratory volume in 1 second (FEV1) of 2740cc (74%), FEV1/FVC ratio of 56% and normal carbon monoxide diffusion (DLCO). Computed tomography (CT) revealed severe bilateral mixed centrilobular and paraseptal pulmonary emphysema, primarily involving the upper lobes, containing frank areas of pulmonary parenchymal destruction and a large paraseptal emphysematous bulla in the anterior segment of the right upper lobe (RUL), longest diameter 9cm (Fig. 1). Given these findings and persisting symptoms, surgical bullectomy was proposed, which the patient refused.
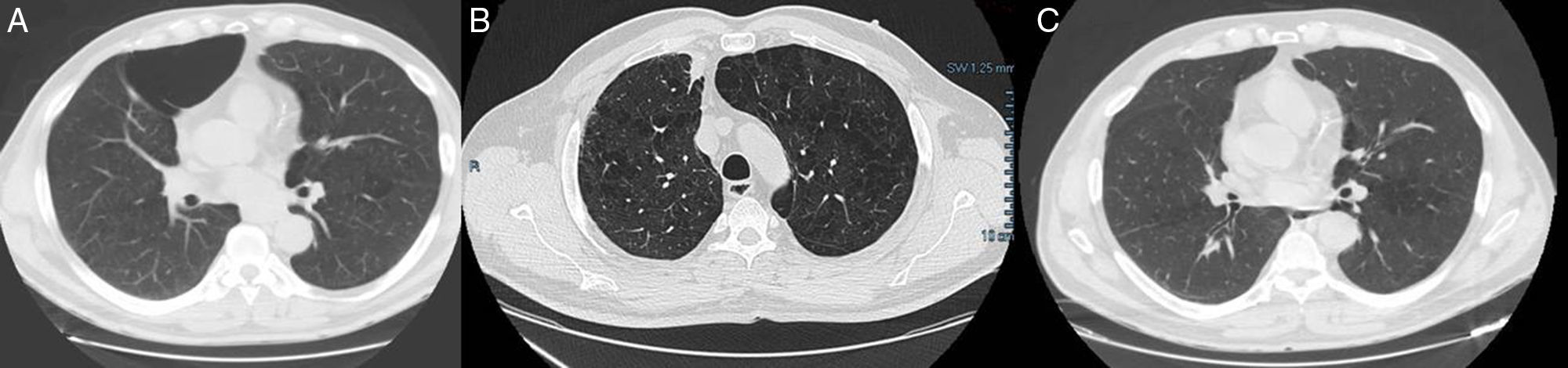
In November 2015, a follow-up chest CT was performed, which revealed a nodular image with slightly spiculated margins in the paramediastinal region of the RUL, in close contact with the fat of the anterior line of pleural reflection, measuring 18×21mm in the anteroposterior and transversal diameter on the axial plane, and 4cm in length on the sagittal plane. Extensive areas of parenchymal pulmonary destruction could still be observed, associated with the prevailing emphysema pattern in the upper lobes. Of particular interest was the disappearance of the large bulla in the anterior segment of the RUL (Fig. 1). Given the suspicion of a malignant solitary pulmonary nodule, a positron emission tomography (PET) was requested that showed a moderately hypermetabolic pulmonary lesions in the RUL, consistent with malignancy, so the lesion was surgically removed. Video-assisted thoracoscopic wedge resection was performed, and pathology study found the lesion to be a residual sclerotic pulmonary nodule, consistent with thrombosed cavernous hemangioma, forming organized dystrophic calcification. In the subsequent lung function tests after resolution of the bulla, no improvement was found on spirometry, with FVC 4600cc (100%), FEV1 2690cc (74%) and a FEV1/FVC ratio of 58%.
As mentioned above, the natural course of bullae is progressive growth, to the extent that giant bullae can become so large that they even cause adjacent parenchyma to collapse.2 Treatment of choice is surgery, which has been shown to improve dyspnea, gas exchange, lung function, and exercise capacity.3 A few cases of spontaneous regression of an emphysematous bulla have been reported, the first of which was probably that published by Douglas and Grant in 1957.4 The process is usually preceded by clinical symptoms consistent with a respiratory infection, manifesting as cough and expectoration, generally with parenchymal consolidation surrounding the bulla and an air-fluid level within. Radiological resolution of air-fluid levels is usually very slow, generally taking more than 70 days, and the use of antibiotics does not speed up the process, so their systematic use is not recommended in asymptomatic patients.5–7 The causative mechanism is unknown, although most authors suggest that it is due to bronchial obstruction by exudate and inflammation, with subsequent reabsorption of the air-fluid content,8 or else it might be an inflammatory process within the bulla which causes it to seal.2 Although in most cases an improvement in lung function has been reported,9 this might not occur, as in the case described by Wahbi and Arnold in 1996,10 and in our patient, possibly due to the size of the bulla.
In our case, the mechanism underlying resolution of the bulla is unclear. At no time was there evidence of inflammatory signs on the CT or previous chest radiographs, making this case unusual, since regression was totally asymptomatic, with no associated infection or tumor. The finding of cavernous hemangioma was incidental, and we do not believe that it is associated with resolution of the bulla.
Please cite this article as: Benito Bernáldez C, Almadana Pacheco V. Regresión espontánea de una bulla enfisematosa pulmonar. Arch Bronconeumol. 2017;53:347–348.







