

Computed tomography (CT)-guided lung aspiration biopsy is a widely used tool in the histopathological diagnosis of lung lesions.1 Although complications from this procedure are rare, they are not unknown, and can include pneumothorax, hemithorax, hemoptysis and/or pulmonary hematoma.
We report the case of a patient who developed pneumothorax and left ventricular air embolism after diagnostic aspiration of a pulmonary nodule.
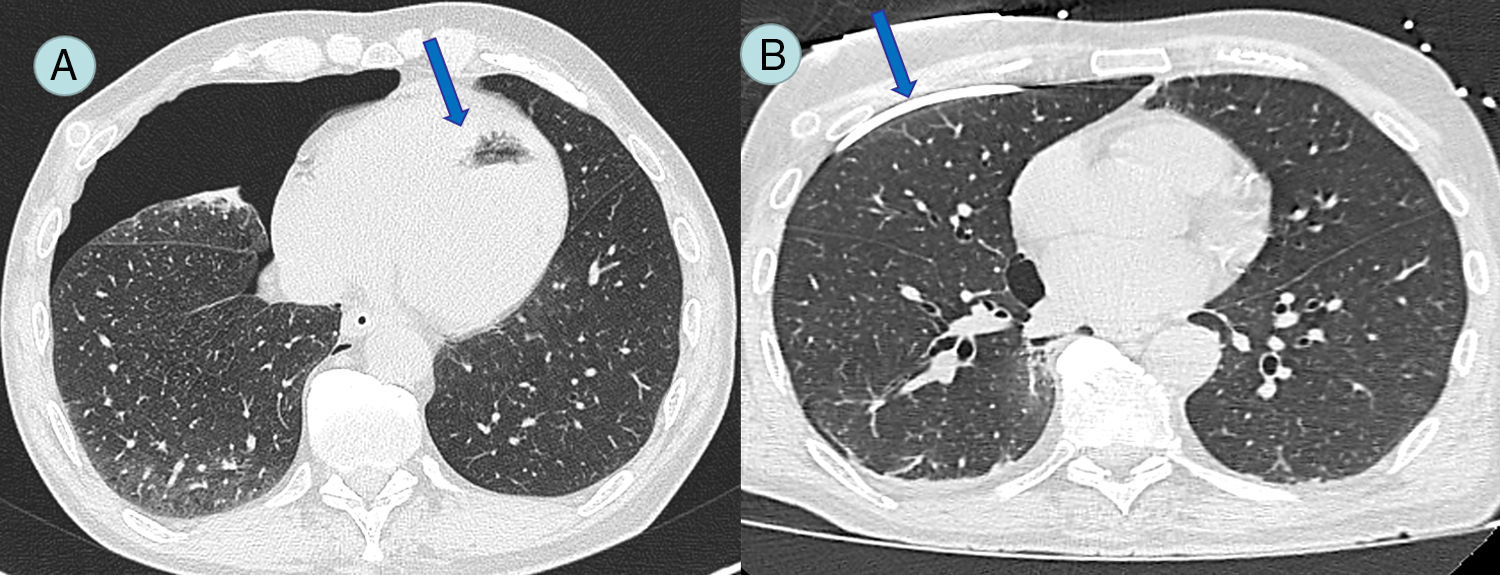
Our patient was a 67-year-old man with a history of perforated colorectal carcinoma, requiring emergency surgery, followed by treatment with chemotherapy and radiation therapy. During the staging CT, a pulmonary nodule measuring 11mm contiguous with the inferior pulmonary vein was observed. Fine needle aspiration biopsy was performed under general anesthesia, and during the procedure pneumothorax and left ventricular air embolism were visualized. This was a tomographic finding, and the patient was asymptomatic when the complication was discovered. A pleural drainage tube was placed, and pulmonary expansion was immediately observed (Fig. 1). Transthoracic echocardiogram was performed, ruling out coronary and/or ventricular complications. A waiting approach was taken, with echocardiographic studies and hemodynamic monitoring, which remained within normal values. A follow-up CT was performed after 48h, showing reabsorption of the intracardiac air. The patient progressed without problems and was discharged on day 4 after the procedure.
CT-guided aspirations are safe procedures with a complication rate of 10%–25%, depending on the series, the most common being pneumothorax. Intracardiac air embolism is an extremely rare and potentially fatal complication, and reports in the literature are few.2
Our patient presented pneumothorax associated with intracardiac air embolism, rarely reported in the literature to date. The proximity of the lesion to the inferior pulmonary vein with the consequent production of intracardiac air embolism is a mechanism known to cause this type of complication.3 Procedures performed under general anesthesia and positive airway ventilation may increase the chances of it occurring.
The therapeutic alternative of using a hyperbaric chamber is controversial, and moreover, unavailable in many hospitals.
Administration of 100% oxygen while placing the patient in the Trendelenburg position, along with intensive hemodynamic monitoring has been shown to be a safe treatment in the management of complications.4,5
Please cite this article as: Dietrich A, Vargas A, Smith DE, Domenech A. Embolia aérea intraventricular como complicación de una punción biopsia pulmonar guiada por tomografía computarizada. Arch Bronconeumol. 2017;53:348–349.







