
Foreign body (FB) aspiration occurs in children less than 3 years old in 75.4% of the total cases of aspirations and bronchoscopic removal presents high potential risk for complications that can lead the patient to death.1
Rigid bronchoscopy has always been advocated as the main choice for tracheobronchial FB's removal2 considering the possibility to provide adequate ventilation during the procedure and the variety of available instruments that can be inserted into the scope. However, in case of migration of the object, the flexible bronchoscopy easily allows exploration of the distal bronchi. For repeated procedures, rigid bronchoscopy might also cause swelling of the vocal cords and laryngeal edema and also for these reasons flexible bronchoscopy raised his popularity in the last years.2–4
In several cases it is difficult to remove FBs in toddlers with flexible bronchoscopy, due to the limited selections of grasping tools capable of passing through the 1.2mm instrument channel of the ultrathin bronchoscope.4,5 Most of the inhaled FBs in children are organic. Their fragility and shape, associated with the presence of inflammatory reaction, makes the use of grasping forceps difficult.5
The wire basket forceps has mainly been used in the urinary duct and biliary tract,4 but we have found this device very useful for foreign body retrieval, in combination with flexible bronchoscopy, in small children aged ≤2 years (12 cases).
We performed the procedure in the operative room, under general anesthesia with an ultrathin flexible bronchoscope (Pentax FB8V 2.8mm) that was introduced through the single-lumen tube. The retrieval basket (Zero Tip Nitinol Stone Retrieval Basket, Boston Scientific 1.9 Fr, 0.63mm×120cm) was inserted through the 1.2mm channel of the scope securely grasping the FB from beside. The basket was then retracted toward the tip of the bronchoscope extracting both through the endotracheal tube.
This tip-less basket allows close FB approximation in the tracheobronchial tree. The flat distal surface eliminates tissue-to-tip interface giving an atraumatic manipulation and the knotted wires give stability to the basket to hold firmly the FB during the extraction. However it is important not to push the device too distally in order to prevent perforation of the bronchi that might easily occur in infants.
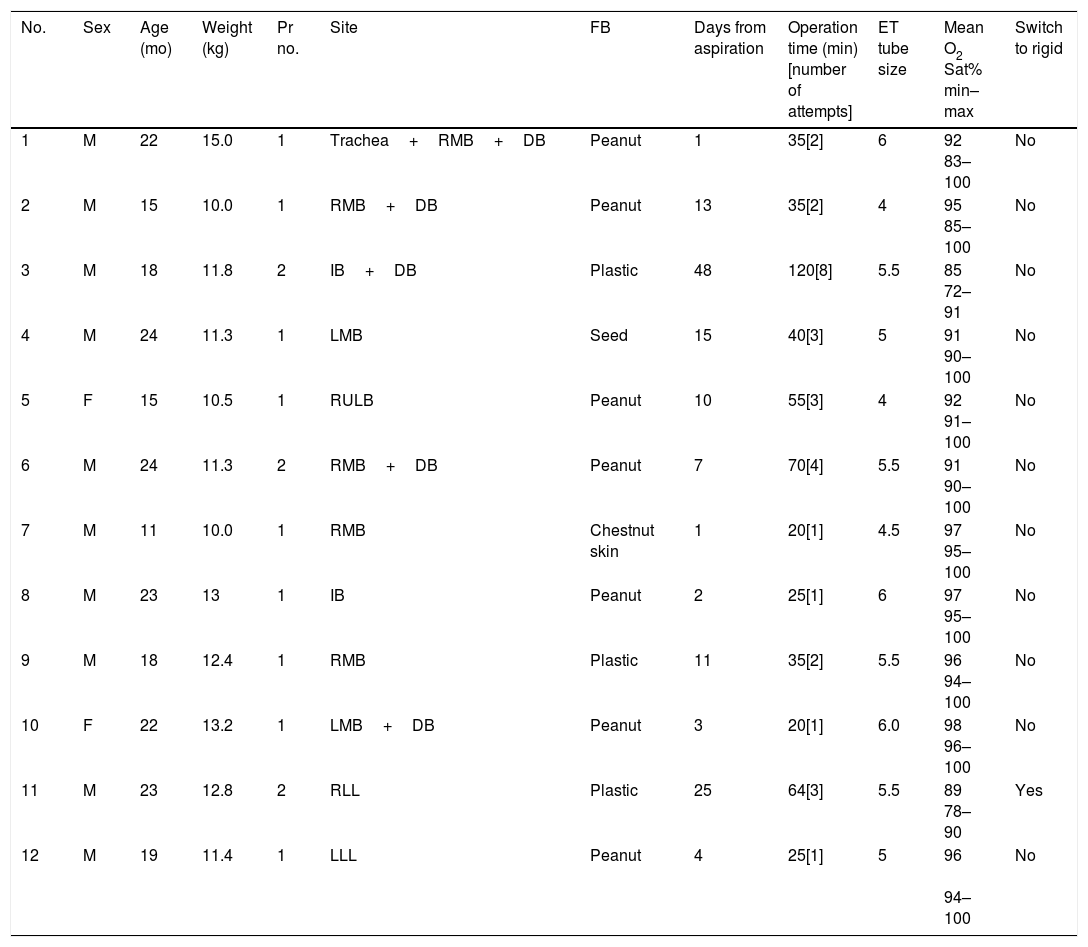
Characteristics of our patients are reported in Table 1. The elapsed time between the aspiration and the endoscopic procedure varied from one to 48 days (mean 11.6±12.8 days). All patients underwent bronchoscopy within few hours from the arrival at the Emergency Room.
Characteristics of the Patients and Intraoperative Data.
| No. | Sex | Age (mo) | Weight (kg) | Pr no. | Site | FB | Days from aspiration | Operation time (min) [number of attempts] | ET tube size | Mean O2 Sat% min–max | Switch to rigid |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 22 | 15.0 | 1 | Trachea+RMB+DB | Peanut | 1 | 35[2] | 6 | 92 83–100 | No |
| 2 | M | 15 | 10.0 | 1 | RMB+DB | Peanut | 13 | 35[2] | 4 | 95 85–100 | No |
| 3 | M | 18 | 11.8 | 2 | IB+DB | Plastic | 48 | 120[8] | 5.5 | 85 72–91 | No |
| 4 | M | 24 | 11.3 | 1 | LMB | Seed | 15 | 40[3] | 5 | 91 90–100 | No |
| 5 | F | 15 | 10.5 | 1 | RULB | Peanut | 10 | 55[3] | 4 | 92 91–100 | No |
| 6 | M | 24 | 11.3 | 2 | RMB+DB | Peanut | 7 | 70[4] | 5.5 | 91 90–100 | No |
| 7 | M | 11 | 10.0 | 1 | RMB | Chestnut skin | 1 | 20[1] | 4.5 | 97 95–100 | No |
| 8 | M | 23 | 13 | 1 | IB | Peanut | 2 | 25[1] | 6 | 97 95–100 | No |
| 9 | M | 18 | 12.4 | 1 | RMB | Plastic | 11 | 35[2] | 5.5 | 96 94–100 | No |
| 10 | F | 22 | 13.2 | 1 | LMB+DB | Peanut | 3 | 20[1] | 6.0 | 98 96–100 | No |
| 11 | M | 23 | 12.8 | 2 | RLL | Plastic | 25 | 64[3] | 5.5 | 89 78–90 | Yes |
| 12 | M | 19 | 11.4 | 1 | LLL | Peanut | 4 | 25[1] | 5 | 96 94–100 | No |
Legend: RMB=right main bronchus; RULB=right upper lobe bronchus; IB=intermediate bronchus; LMB=left main bronchus; DB=distal bronchi; LLL=left lower bronchus; Pr no.=number of procedures; FB=foreign body.
Three patients underwent two bronchoscopies in seven days due to the strong inflammatory reaction around the FB that jeopardized its removal on a first attempt (patients 3, 6 and 11). Mean operative time was 45.3±27.5min (range 20–120min). Patients undergoing a second procedure required a longer operative time, due also to different attempts of FB's removal with different grasping forceps, before being able to finally retrieve the objects by mean of the urologic basket. Number of attempts during the procedure varied from 1 to 8 (mean 2.5±1.8). In one patient (patient 11) switch to rigid bronchoscope has been necessary due to the small dimension of the toy's piece of plastic that would slipper away from the urologic basket.
O2 saturation was stable in all procedures (mean 93.2%±3.7mmHg) and it fell below 90% in patient 1,2, 3 and 11, the last two requiring to be re-intubated during the FB's removal
Complications occurred in patient 3 and consisted of post-extubating bronchospasm controlled with medical therapy. The longest interval between FB's aspiration and its removal was correlated with the onset of postoperative complication in patient 3 and 11.
Although some authors prefer the association of rigid and flexible bronchoscopy,2 our preferred choice is the flexible bronchoscopy through endobronchial tube, when FB aspiration is likely to have occurred more than 48h before. This is due to the fact that a strong inflammatory reaction in the bronchi might lead to the necessity of repeated procedures and though repeated intubations. Nevertheless, rigid bronchoscopy should be always available in the operative room (as in patient 11) and the surgical team should be qualified and ready also to switch to any surgical option.
We advocate this procedure in small children because the use of an ultrathin bronchoscope through the endotracheal tube allows more space ventilation and the combination with the tip-less urology stone retrieval basket increases the percentage of success reducing the risk of tracheobronchial tree trauma.







