
Identification of suitable biomarkers that facilitate the screening and evaluation of pediatric obstructive sleep apnea (OSA) and its severity was explored.
MethodsData-independent acquisition quantitative proteomic analysis was employed to identify serum and urine proteins with differential expression patterns between children with OSA and controls. Differentially expressed proteins that gradually increased or decreased with the severity of OSA were retained as potential biomarkers and underwent ELISA validation.
ResultsWe found that with increasing severity of OSA, there was a gradual upregulation of 34 proteins in the serum and 124 proteins in the urine, along with a respective downregulation of 10 serum proteins and 64 urinary proteins in the initial cohort of 40 children. These proteins primarily participate in immune activation, the complement pathway, oxygen transport, and reactive oxygen metabolism. Notably, cathepsin Z exhibited a positive correlation with the obstructive apnea hypopnea index, whereas sex hormone-binding globulin (SHBG) was negatively correlated. These proteins were then validated by ELISA in an independent cohort (n=21). Circulating cathepsin Z and SHBG levels displayed acceptable diagnostic performance of OSA with AUC values of 0.863 and 0.738, respectively.
ConclusionsWe identified two promising circulating proteins as novel biomarkers for clinical diagnosis and assessment of pediatric OSA severity. Furthermore, the comprehensive proteomic profile in pediatric OSA should aid in exploring the underlying pathophysiological mechanisms associated with this prevalent condition.

Pediatric obstructive sleep apnea (OSA) is characterized by recurrent increases in upper airway resistance during sleep, resulting in increased respiratory efforts along with impaired ventilation and sleep quality. This prevalent condition leads to intermittent hypoxia, hypercapnia, fragmented sleep as well as altered autonomic nervous system function, oxidative stress, and systemic inflammation.1,2 Consequently, a cascade of pathophysiological processes may occur and detrimentally affect the central nervous, cardiovascular, and endocrine systems.3 The prevalence of childhood OSA is unclear but estimated to range from 1.2% to 5.7% worldwide.4 Currently, overnight polysomnography (PSG) serves as the diagnostic gold standard for pediatric OSA, with disease severity typically assessed using the obstructive apnea hypopnea index (OAHI). However, the limited accessibility and high cost of PSG hinder its widespread application and impose substantial delays in diagnosis and treatment.5 If early screening for pediatric OSA can be conducted through implementation of clinical biomarkers in serum or urine thereby enabling timely risk stratification and targeted therapeutic interventions, it would likely improve the prognosis of affected children. Currently, promising biomarkers for adult OSA include interleukin-6, tumor necrosis factor-α and high sensitivity C-reactive protein.6 In a systematic review of the cardiovascular risks of pediatric OSA, it was shown that the expression levels of biomarkers such as natriuretic peptide, endothelin-1 and adiponectin decrease significantly after tonsillectomy, suggesting that cardiovascular risks are associated with OSA. This observation indicates that these proteins are biomarkers of vascular damage in the context of children with OSA, guiding the risk stratification of disease and long-term follow-up of postoperative cardiovascular risk.
Data-independent acquisition (DIA) is an unbiased mass spectrometry (MS) method that enables comprehensive scanning of all ions in a sample. DIA enables more comprehensive data acquisition, thereby capturing all MS signals within samples while reducing inter-analysis variability, which facilitates robust quantitative and comparative analyses. Protein biomarker analysis has been used widely in diagnosing various diseases, including7 Alzheimer's disease8 diabetes, and9 cancer.10,11 Recent studies have highlighted the correlation between several serum proteins, such as ROBO3, tPA and LG3BP, and the severity of adult OSA, suggesting their potential as diagnostic biomarkers. However, pediatric OSA has distinct etiology and clinical symptoms compared to its adult counterpart.12,13 Efforts to identify potential serum and urinary biomarkers of OSA in children have yielded heterogeneous results, such that no validated serum or urine biomarkers have been proposed for assessing the severity of pediatric OSA. In this study, we used DIA to identify potential biomarkers associated with standard clinical severity indicators of pediatric OSA in the serum and urine of children. The preliminary findings were then validated through ELISA detection of candidate proteins using an independent sample set.
MethodsParticipant InformationWe recruited 28 pediatric OSA patients admitted to Beijing Children's Hospital, Capital Medical University. Inclusion criteria: (1) ages 3–11 years old; and (2) have symptoms of snoring or mouth opening with an OAHI>1event/h on PSG. Exclusion criteria: (1) those with craniofacial abnormalities, such as Down syndrome and Crouzon syndrome; (2) genetic metabolic disorders and neuromuscular diseases; (3) endocrine disorders, renal diseases, autoimmune diseases; (4) obese children, i.e., body mass index (BMI)>95th percentile for children of the same age and sex; and (5) upper respiratory infection in the last two weeks. Among them, 10 were mild OSA (male, 50%; mean age, 5.31±1.00 years), 9 were designated as moderate OSA (male, 66.7%; mean age, 6.37±2.33 years) and 9 children suffered from severe OSA (male, 44.4%; mean age, 4.92±0.92 years).
Twelve children who had pigmented nevus in the dermatology ward formed the control group (male, 58.3%; mean age, 5.77±1.55 years). They had no history of snoring or open-mouth breathing, tonsillar enlargement and were matched to the OSA groups for age, sex and BMI. The guardians of all participants signed an informed consent form. The study protocol was approved by the Ethics Committee of Beijing Children's Hospital.
PolysomnographyA standard overnight attended PSG was performed using Compumedics E-series (Compumedics, Australia) and Alice 5 (Respironics, Murrysville, PA, USA). Children were instructed to fall asleep naturally, refraining from consuming coffee, tea, cola or sedative-hypnotic drugs prior to sleep onset, with monitoring duration of the study exceeding 7h. PSG monitoring included six-channel electroencephalography (F3/M2, F4/M1, C3/M2, C4/M1, O1/M2, O2/M1), electrooculography, electromyography of the submental muscles, anterior tibialis electromyography, electrocardiography, thoracoabdominal respiratory movements, transcutaneous oxygen saturation, airflow (thermistor and pressure sensors), snoring sensor and body position.14 Sleep staging and event scoring were manually performed by experienced pediatric PSG technicians at the sleep center, according to the scoring manual published by the American Academy of Sleep Medicine. The OAHI refers to the average number of obstructive apneas, mixed apneas and obstructive hypopneas per hour of total sleep time.15 Children were categorized as mild, moderate or severe OSA based on their OAHI (mild OSA: >1 and ≤5events/hour sleep (e/h); moderate OSA: >5 and ≤10e/h; severe OSA: ≥10e/h).
Serum and urine sample collectionBlood and urine samples from children with OSA were collected in the morning after PSG monitoring, whereas samples from the control group were collected the morning after admission. Fasting blood specimens (∼5ml) were obtained using non-anticoagulant tubes and allowed to coagulate for 30min. After coagulation, the tubes were centrifuged at 3000×g and 4°C for 3min. The upper serum layer was isolated and stored at −80°C until analysis. Urine samples (∼10ml of midstream morning urine) were collected using centrifuge tubes. Urine samples were centrifuged at 3000×g and 4°C for 15min to remove cellular debris and impurities, and the resulting supernatants were stored at −80°C for subsequent analysis.
Total protein extractionSerum samples were treated with urea until fully dissolved, then centrifuged at 14,000×g for 20min to collect supernatants. Ten microliters were aliquoted for Bradford protein quantification, and the remaining samples were stored at −80°C. Urine samples were dissolved at 37°C, centrifuged at 2000×g for 10min, and 1ml of supernatant was collected. Urea was added to a final concentration of 8mol/L, and the samples were loaded onto 10kDa ultrafiltration units (Millipore, MA, USA), centrifuged at 14,000×g, and concentrated to 0.1ml. The concentrated urine protein was collected, and Bradford protein quantification was performed.
Peptide preparationEach sample containing 100μg protein underwent reduction with 10mm DTT at 56°C for 1h, followed by alkylation with iodoacetamide. Trypsin digestion was performed for 16h at room temperature. A portion of peptides from each sample was combined to create a pooled sample, while the remaining peptides were analyzed individually.16 Desalting of pooled and individual peptide samples with excess urea was carried out using a C18 cartridge-based method, followed by vacuum centrifugation drying (RT, 1500rpm).
Library constructionThe combined sample was separated using a Waters BEH C18 column (4.6mm×250mm, 5μm) attached to a Rigol L3000 HPLC system (Rigol, China). Shotgun proteomics were performed using a Thermo Fisher U3000 ultra-high performance liquid chromatography (UHPLC) system and an Orbitrap Fusion MS in data-dependent acquisition (DDA) mode. Full-scan mass spectra (m/z 250 to 1450, resolution 120,000) were acquired, followed by data-dependent MS/MS scans. Collision energy was normalized to 30% using HCD fragmentation.
Data-independent acquisitionIndividual samples were mixed with 0.2μl standard peptides from the iRT kit by Biognosys (Zurich, Switzerland) and loaded onto the U3000 UHPLC system attached to an Orbitrap Fusion MS (Thermo Fisher) operating in DIA mode. Chromatographic conditions mirrored those previously described. The MS was programmed with MS1 resolution at 120,000 and MS2 resolution at 30,000, acquiring spectra from m/z 350 to 1350. Additional DIA parameters included a normalized collision energy of 35% and a target value for resulting MS2 spectra.
Gene ontology enrichment analysisProteins displaying differential expression were examined using the Gene Ontology (GO) database (www.geneontology.org). Accordingly, significant pathways required at least three shared elements among the analyzed genes, and a stringent p-value threshold of ≤0.01 was used to establish robust statistical significance.
Experimental verification (ELISA)Further validation of the accuracy of biomarkers was achieved by selecting differentially expressed proteins in serum and urine that correlated strongest with the severity of OSA, along with proteins that gradually increased or decreased with the severity of the disease (namely, calbindin Z and sex hormone-binding globulin (SHBG)). Because of the limited number of blood samples, we randomly selected two individuals from the mild group, three from the moderate group and four from the severe group from the original cohort. Additionally, for biomarker validation, we recruited five children for the control group, four for the mild OSA and three for the severe OSA, resulting in a total of five individuals in the control group, six in the mild group, three in the moderate group and seven in the severe group. Furthermore, the clinical characteristics and PSG results of the selected validation cases are largely consistent with those in the proteomic analysis. Serum and urine samples were tested by ELISA kits (Human Cathepsin Z ELISA Kit ab287165, Abcam (Shanghai) TRADING Co., LTD, China, Sensitivity: 2.48pg/ml, Range: 10.94–700pg/ml; Human SHBG ELISA Kit ab260070, Abcam (Shanghai) TRADING Co., LTD, China, Sensitivity: 26pg/ml, Range: 62.5–4000pg/ml) according to the manufacturer's instructions. The corresponding kits were balanced to room temperature, and after washing, the samples and standard solutions were added and incubated at room temperature for 2h. After washing five times, the corresponding enzyme-labeled secondary antibodies were added and incubated at room temperature for 1h. Finally, the substrate and chromogenic agent were added, and the absorbance (D) value at 450nm was detected using an ELISA reader.
Statistical analysisStatistical analysis was performed using R software (version 4.2.2). Normally distributed quantitative data are represented by the mean and standard deviation, indicating central tendency and variability. One-way ANOVA was used to detect significant group variations. Protein level differences among groups were assessed using the two-sided t-test. For non-normally distributed metric data, we present these data using the median and quartiles and perform comparisons using the non-parametric Kruskal–Wallis test. Count data, often as percentages, were examined via the chi-square test to identify associations and deviations. A significance threshold of p<0.05 was used.
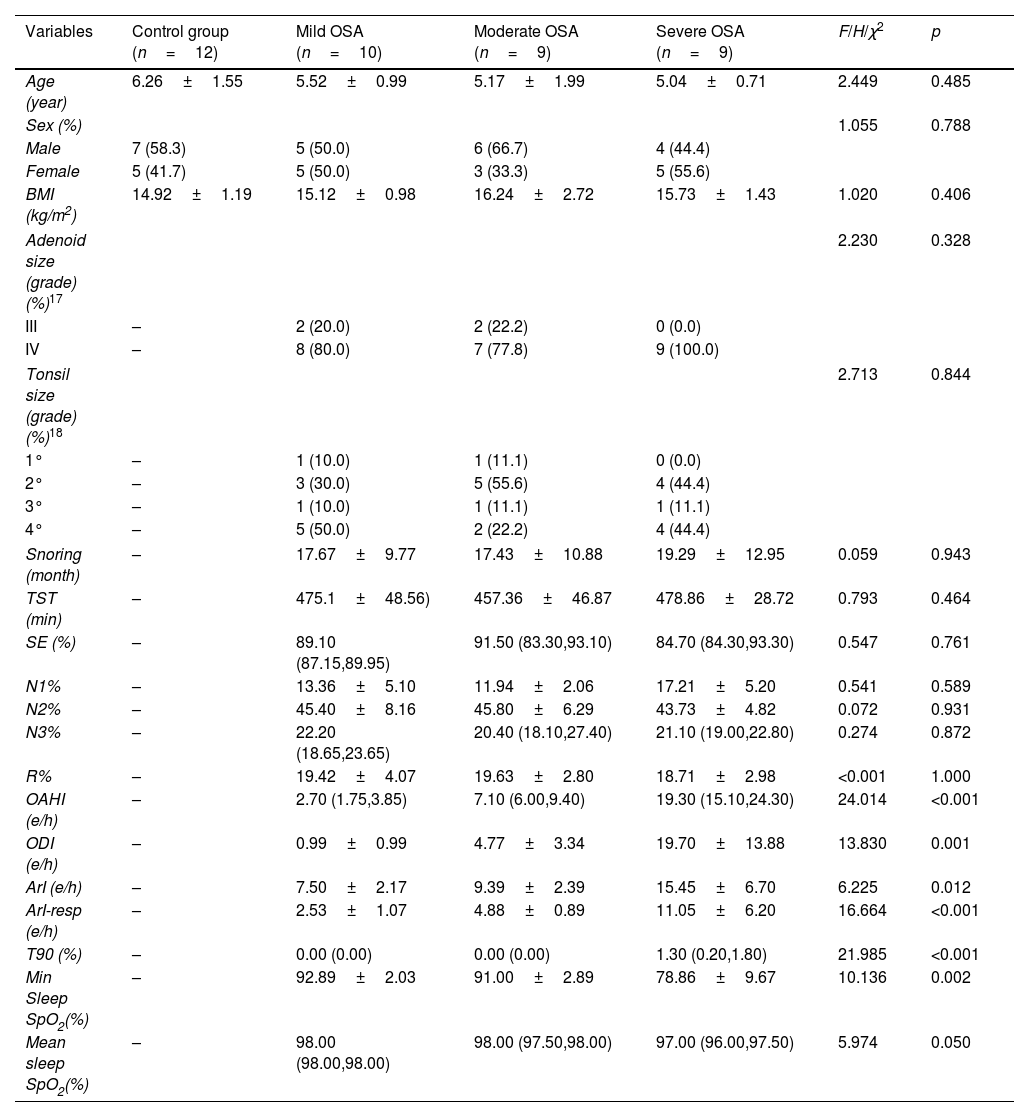
ResultsBasic clinical featuresNo differences in age, sex and BMI were present across severity groups (p>0.05). There were no significant differences (p>0.05) in adenoid and tonsil size, total sleep time and time spent in each sleep stage among the mild, moderate and severe OSA groups. As expected, the OAHI and ODI increased gradually with the severity of OSA. Minimum oxygen saturation (SpO2) and mean SpO2 decreased as the severity of OSA increased (Table 1).
Clinical characteristics and PSG results.
| Variables | Control group (n=12) | Mild OSA (n=10) | Moderate OSA (n=9) | Severe OSA (n=9) | F/H/χ2 | p |
|---|---|---|---|---|---|---|
| Age (year) | 6.26±1.55 | 5.52±0.99 | 5.17±1.99 | 5.04±0.71 | 2.449 | 0.485 |
| Sex (%) | 1.055 | 0.788 | ||||
| Male | 7 (58.3) | 5 (50.0) | 6 (66.7) | 4 (44.4) | ||
| Female | 5 (41.7) | 5 (50.0) | 3 (33.3) | 5 (55.6) | ||
| BMI (kg/m2) | 14.92±1.19 | 15.12±0.98 | 16.24±2.72 | 15.73±1.43 | 1.020 | 0.406 |
| Adenoid size (grade) (%)17 | 2.230 | 0.328 | ||||
| III | – | 2 (20.0) | 2 (22.2) | 0 (0.0) | ||
| IV | – | 8 (80.0) | 7 (77.8) | 9 (100.0) | ||
| Tonsil size (grade) (%)18 | 2.713 | 0.844 | ||||
| 1° | – | 1 (10.0) | 1 (11.1) | 0 (0.0) | ||
| 2° | – | 3 (30.0) | 5 (55.6) | 4 (44.4) | ||
| 3° | – | 1 (10.0) | 1 (11.1) | 1 (11.1) | ||
| 4° | – | 5 (50.0) | 2 (22.2) | 4 (44.4) | ||
| Snoring (month) | – | 17.67±9.77 | 17.43±10.88 | 19.29±12.95 | 0.059 | 0.943 |
| TST (min) | – | 475.1±48.56) | 457.36±46.87 | 478.86±28.72 | 0.793 | 0.464 |
| SE (%) | – | 89.10 (87.15,89.95) | 91.50 (83.30,93.10) | 84.70 (84.30,93.30) | 0.547 | 0.761 |
| N1% | – | 13.36±5.10 | 11.94±2.06 | 17.21±5.20 | 0.541 | 0.589 |
| N2% | – | 45.40±8.16 | 45.80±6.29 | 43.73±4.82 | 0.072 | 0.931 |
| N3% | – | 22.20 (18.65,23.65) | 20.40 (18.10,27.40) | 21.10 (19.00,22.80) | 0.274 | 0.872 |
| R% | – | 19.42±4.07 | 19.63±2.80 | 18.71±2.98 | <0.001 | 1.000 |
| OAHI (e/h) | – | 2.70 (1.75,3.85) | 7.10 (6.00,9.40) | 19.30 (15.10,24.30) | 24.014 | <0.001 |
| ODI (e/h) | – | 0.99±0.99 | 4.77±3.34 | 19.70±13.88 | 13.830 | 0.001 |
| ArI (e/h) | – | 7.50±2.17 | 9.39±2.39 | 15.45±6.70 | 6.225 | 0.012 |
| ArI-resp (e/h) | – | 2.53±1.07 | 4.88±0.89 | 11.05±6.20 | 16.664 | <0.001 |
| T90 (%) | – | 0.00 (0.00) | 0.00 (0.00) | 1.30 (0.20,1.80) | 21.985 | <0.001 |
| Min Sleep SpO2(%) | – | 92.89±2.03 | 91.00±2.89 | 78.86±9.67 | 10.136 | 0.002 |
| Mean sleep SpO2(%) | – | 98.00 (98.00,98.00) | 98.00 (97.50,98.00) | 97.00 (96.00,97.50) | 5.974 | 0.050 |
Abbreviations: BMI, body mass index; TST, total sleep time; SE%, sleep efficiency; N1%, N2%, N3% and R%, percentage of non-REM sleep stage 1, 2 and 3 and REM sleep stage of total sleep time, respectively; OAHI, obstructive apnea–hypopnea index; ODI, oxygen desaturation index; ArI, arousal index; ArI-resp., respiratory related arousal index; T90, the proportion of total sleep time with oxygen saturation<90%; SpO2, oxygen saturation.
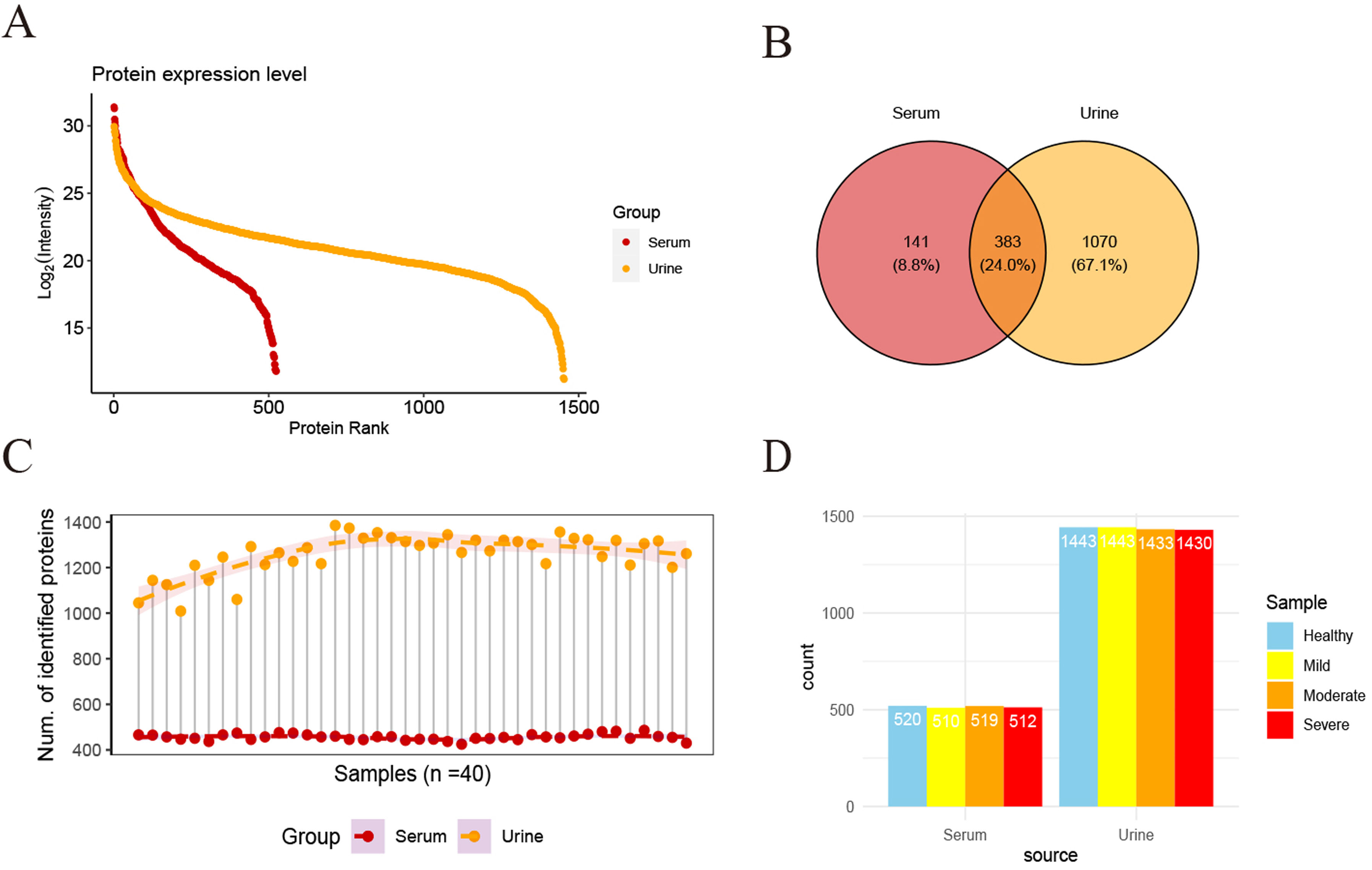
For all serum and urine samples among the 40 subjects, 524 serum proteins and 1453 urine proteins were identified. From the identified proteins, 383 proteins were found to be present in both serum and urine (Fig. 1A, B). Moreover, the protein abundance distribution in each sample/group was consistent (Fig. 1C, D).
 Using mass spectrometry to analyze serum and urine samples, a total of 524 and 1453 proteins were detected in serum and urine, respectively. (B) Co-expression of protein species in serum and urine. (C) Serum and urine protein expression levels in each sample. (D) Protein expression levels in serum and urine in each group.")
Overall proteome. (A) Using mass spectrometry to analyze serum and urine samples, a total of 524 and 1453 proteins were detected in serum and urine, respectively. (B) Co-expression of protein species in serum and urine. (C) Serum and urine protein expression levels in each sample. (D) Protein expression levels in serum and urine in each group.
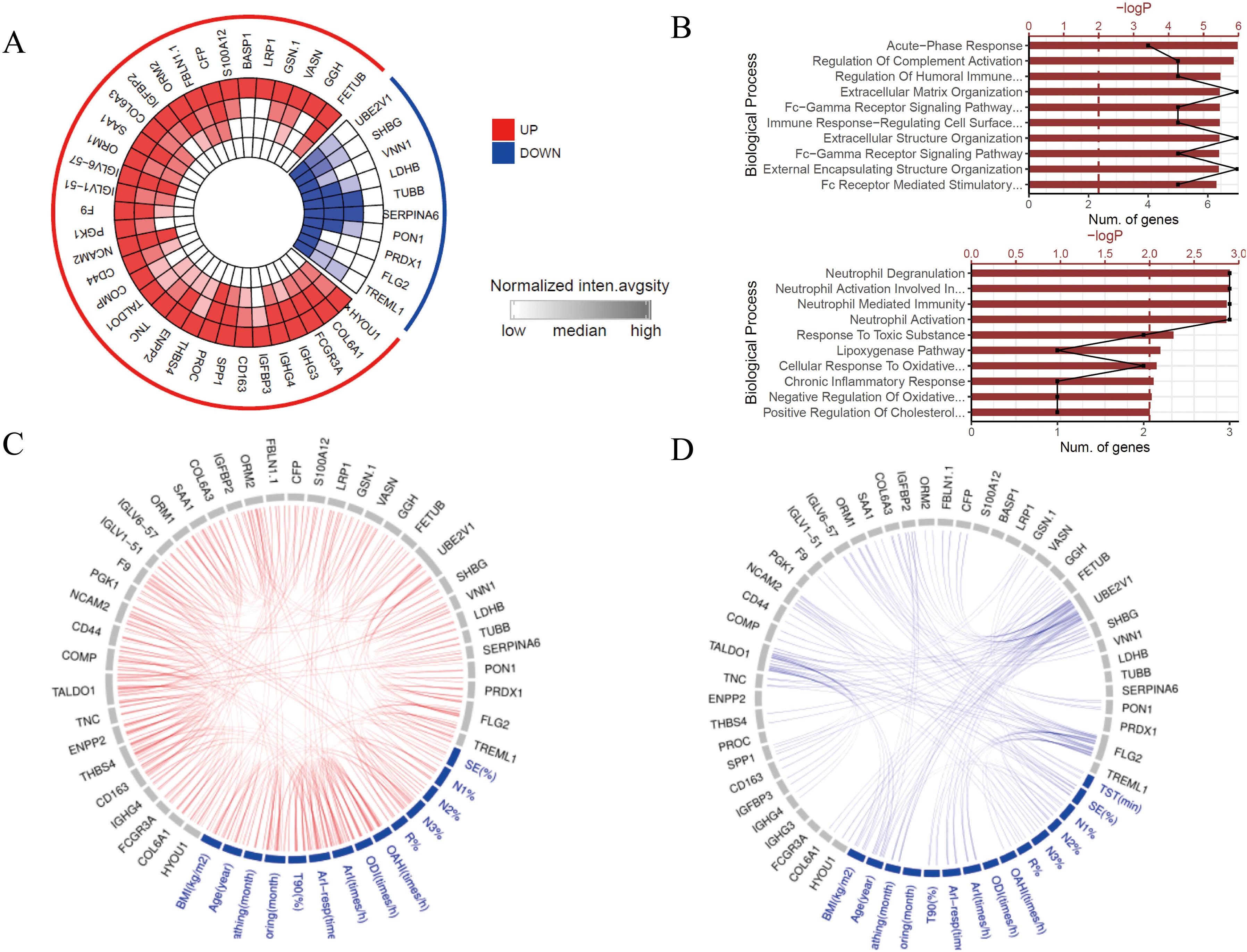
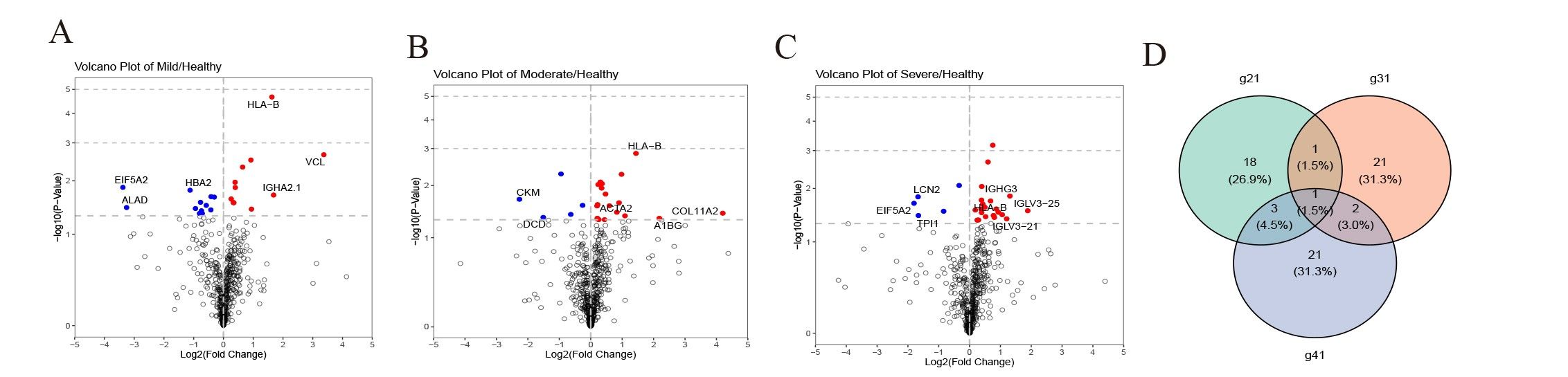
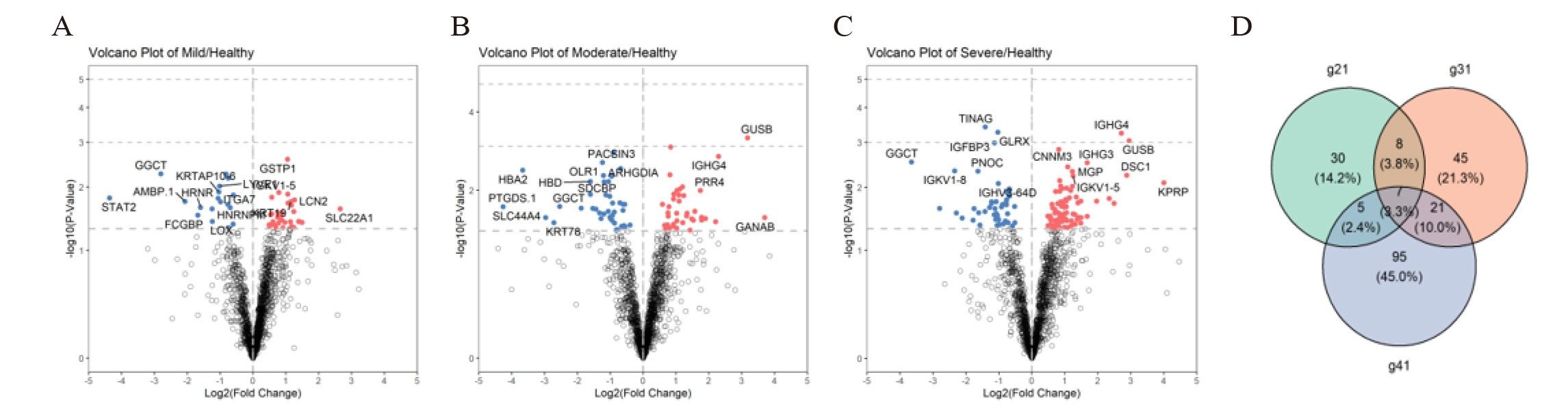
There were 23, 25, and 27 differentially expressed proteins in the serum of the control group compared to the mild, moderate and severe groups, respectively (Supplementary Fig. 1A–D). There were 34 proteins that exhibited progressively higher expression and 10 with progressively lower expression as the severity of OSA increased (Fig. 2A). Upregulated proteins were mainly enriched in functions such as acute-phase response, complement activation and regulation of the humoral immune response. Downregulated proteins were mainly enriched in functions such as neutrophil degranulation, cellular response to oxidative stress and the steroid metabolic process (Fig. 2B). Differentially expressed proteins, including cathepsin Z, COMP and IGHG4, correlated positively with OSA clinical indicators such as OAHI, ODI and ArI. Proteins that correlated negatively with these indicators included SHBG, UBE2V1 and FLG2 (Fig. 2C, D).
 Proteins with progressively up- and downregulation with increasing severity of OSA in serum. The inner to outer circles represent the control group, mild OSA, moderate OSA and severe OSA. Red indicates an increase in protein expression levels, whereas blue represents a decrease. The depth of color reflects the expression level of a protein. (B) Functional enrichment of proteins with progressively higher and lower OSA severity. (C) Differentially expressed proteins that show a positive correlation with the clinical indicators. Nodes represent proteins or clinical indicators, with node size indicating the degree of correlation and edges representing their interactions. (D) Differentially expressed proteins that show a negative correlation with the clinical indicators.")
Serum proteomic profile. (A) Proteins with progressively up- and downregulation with increasing severity of OSA in serum. The inner to outer circles represent the control group, mild OSA, moderate OSA and severe OSA. Red indicates an increase in protein expression levels, whereas blue represents a decrease. The depth of color reflects the expression level of a protein. (B) Functional enrichment of proteins with progressively higher and lower OSA severity. (C) Differentially expressed proteins that show a positive correlation with the clinical indicators. Nodes represent proteins or clinical indicators, with node size indicating the degree of correlation and edges representing their interactions. (D) Differentially expressed proteins that show a negative correlation with the clinical indicators.
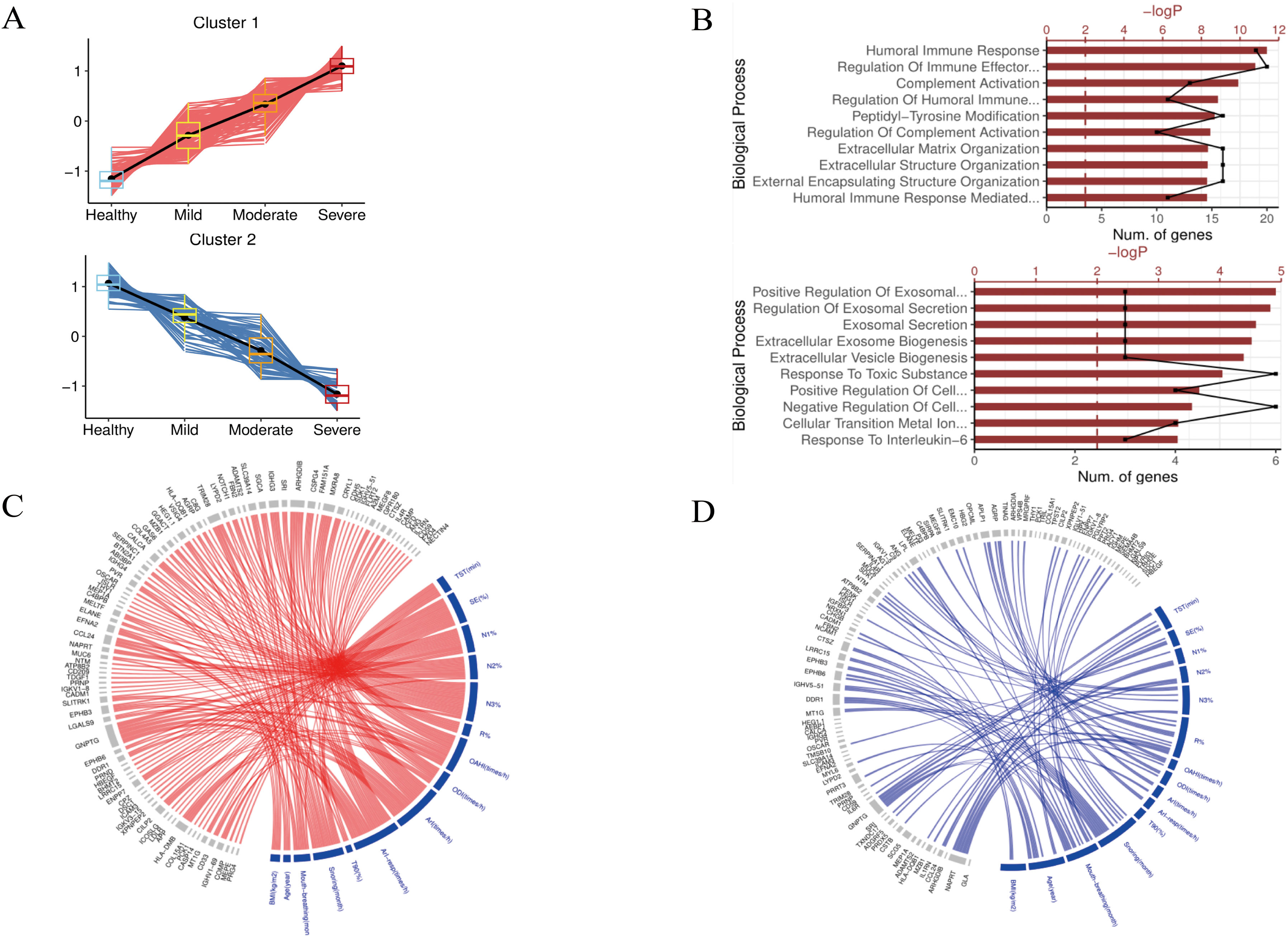
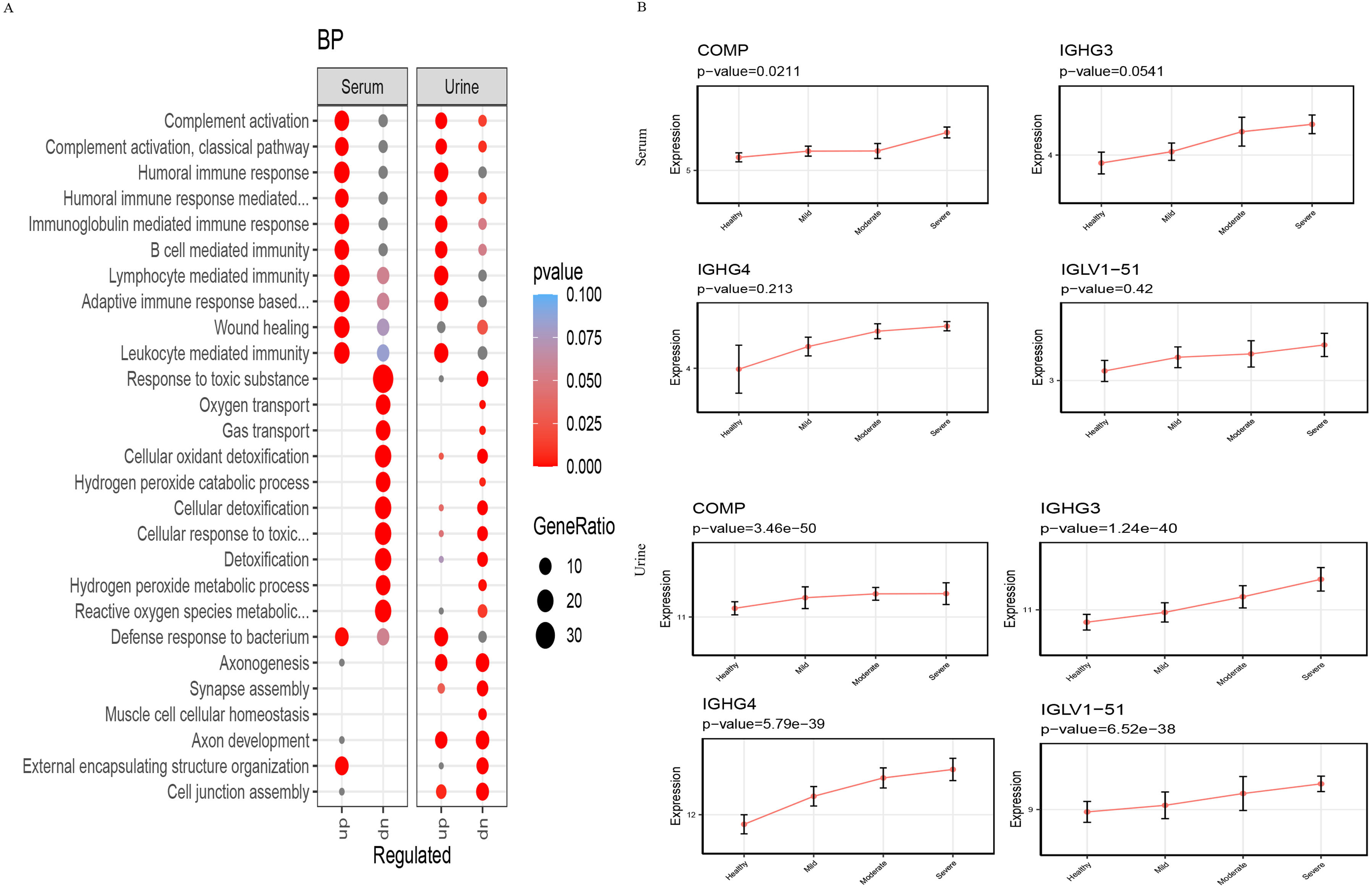
There were 50, 81 and 128 differentially expressed proteins in the urine of the control children compared to the mild, moderate and severe OSA groups, respectively (Supplementary Fig. 2A–D). There were 124 proteins with progressively higher expression as the severity of OSA increased, and 64 proteins with progressively lower expression as the severity of OSA increased (Fig. 3A). Upregulated proteins were mainly enriched in the humoral immune response, regulation of chemokine production and neutrophil-mediated immunity. Downregulated proteins were mainly enriched in exosomal secretion, cellular oxidant detoxification and regulation of T cell activation (Fig. 3B). Differentially expressed proteins, including cathepsin Z, GNPTG and IGHG3, correlated positively with OSA clinical indicators such as OAHI, ODI and ArI. Several proteins correlated negatively with indicators, including SHBG, DDR1 and EPHB3 (Fig. 3C, D).
 Proteins with progressively higher and lower expression levels with increasing severity of OSA in urine. (B) Functional enrichment of proteins with progressively higher and lower OSA severity. (C) Differentially expressed proteins that show a positive correlation with the clinical indicators. (D) Differentially expressed proteins that show a negative correlation with the clinical indicators.")
Urine proteomic profile. (A) Proteins with progressively higher and lower expression levels with increasing severity of OSA in urine. (B) Functional enrichment of proteins with progressively higher and lower OSA severity. (C) Differentially expressed proteins that show a positive correlation with the clinical indicators. (D) Differentially expressed proteins that show a negative correlation with the clinical indicators.
The identified upregulated proteins in serum and urine samples are mainly involved in functions such as humoral immune activation and complement activation. In contrast, those proteins that are downregulated are mainly involved in functions such as oxygen transport and reactive oxygen metabolism (Fig. 4A). Proteins that were identified to be simultaneously upregulated with OSA severity in serum and urine are IGHG3, IGHG4, COMP and IGLV1-51 (Fig. 4B).
Experimental verification Function of differential proteins in serum and urine. (B) Proteins progressively upregulated with OSA severity in serum and urine.")
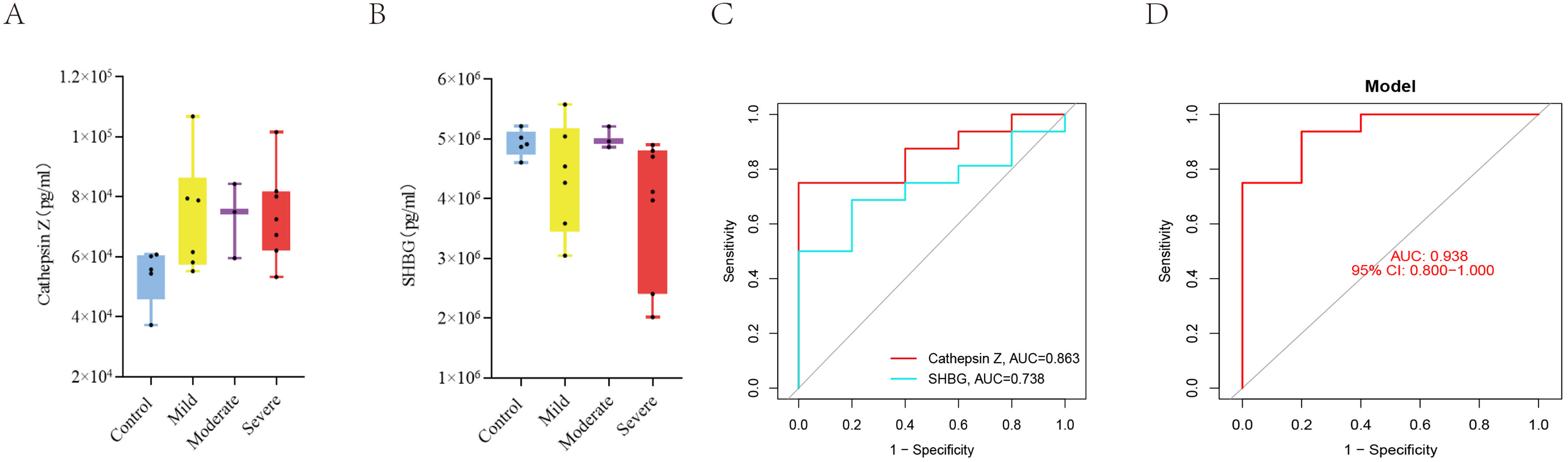
We examined the expression of cathepsin Z and SHBG in the serum of a separate cohort of children and found that cathepsin Z expression increased as the severity of OSA increased, whereas SHBG expression decreased as the severity of OSA increased (Fig. 5A, B). ROC curves were generated based on ELISA results from the validation group. Therefore, the expression levels of cathepsin Z and SHBG in serum exhibit acceptable diagnostic performance for pediatric OSA, with ROC-AUC values of 0.863 and 0.738, sensitivities of 0.75 and 0.69, and specificities of 1 and 0.8, respectively (Fig. 5C, Supplementary Table 1). The ROC-AUC for the combined diagnosis of pediatric OSA using cathepsin Z and SHBG was 0.938, with a sensitivity of 0.75 and a specificity of 1 (Fig. 5D, Supplementary Table 1).
 Expression of cathepsin Z correlates positively with OSA severity. (B) Expression of SHBG correlates negatively with OSA severity. (C) ROC curves for the separate diagnosis of pediatric OSA using the expression levels of cathepsin Z and SHBG in serum. (D) ROC curves for the combined diagnosis of pediatric OSA using cathepsin Z and SHBG in serum.")
Experimental verification. (A) Expression of cathepsin Z correlates positively with OSA severity. (B) Expression of SHBG correlates negatively with OSA severity. (C) ROC curves for the separate diagnosis of pediatric OSA using the expression levels of cathepsin Z and SHBG in serum. (D) ROC curves for the combined diagnosis of pediatric OSA using cathepsin Z and SHBG in serum.
OSA is a serious childhood breathing disorder during sleep with a high prevalence leading to growing concerns about its detection and timely treatment.19 Diagnosis primarily relies on costly overnight PSG testing in specialized centers with severity being appraised through several of the PSG-related measures such as OAHI. Identifying biomarkers for early OSA diagnosis and its severity is therefore important. We used DIA MS-based quantitive proteomics to detect serum and urine proteins that would be differentially expressed in OSA patients and identified potential biomarkers linked to OSA severity through clinical indicator correlations. Our major findings reveal that the differentially expressed proteins were primarily enriched in functions related to neutrophil-mediated immunity, steroid metabolism and other associated pathways. Notably, cathepsin Z and SHBG which are known to participate in these functions, exhibited close associations with the severity of OSA, thereby offering new prospective avenues for investigation into the pathogenesis and diagnosis of OSA.
In the serum samples, 524 proteins were identified, whereas in the urine samples, we detected 1453 proteins.20 The number of identified proteins in serum and urine samples was consistent with previous studies involving children. Based on serum proteomics, our results revealed that the expression of 34 proteins gradually increased as the severity of OSA increased, whereas the expression of 10 proteins showed gradual decreases. Similarly, in urine samples, the expression of 124 proteins displayed progressive increments with increasing OSA severity, whereas 64 proteins exhibited gradual decreases. Importantly, the differentially-regulated proteins in the serum and urine exhibited functional consistency. Indeed, upregulated proteins were primarily involved in humoral immunity and complement activation, whereas the downregulated proteins were mainly associated with oxygen transport and reactive oxygen metabolism.21,22 We postulate that these pathways as revealed by the candidate proteins may be associated with systemic chronic inflammation and oxidative stress in OSA patients.23 OSA has now been extensively identified as a chronic disease that induces systemic oxidative stress and inflammation, thereby promoting the expression of cytokines and adhesion molecules. Previous studies have shown that OSA patients exhibit significant increases in apoptosis and macrophage activation markers compared to controls, and the severity of OSA is positively correlated with the degree of inflammation.23 Inflammatory markers commonly associated with OSA include C-reactive protein, tumor necrosis factor-α and interleukin-6.24,25 Furthermore, OSA in children can increase catecholamine levels, which in turn can promote platelet aggregation and induce a hypercoagulable state.26,27 The classical pathway of complement activation triggers a cascade reaction, inducing a systemic inflammatory response. In this study, numerous proteins in serum and urine samples were upregulated and associated with chronic inflammation. These findings provide further support to further exploration of inflammation-related biomarkers in pediatric OSA as indicator of the presence of the disease as well as the underlying morbidities of pediatric OSA.28 Oxidative stress is characterized by a sharp increase in reactive oxygen species (ROS) levels under certain circumstances, surpassing the antioxidant capacity.29 The intermittent periods of hypoxemia followed by reoxygenation can trigger the generation of ROS, thereby inducing systemic oxidative stress. OSA patients may exhibit higher levels of oxygen free radicals and lower antioxidant status in their plasma.29 The imbalance between the production of oxygen free radicals and antioxidant capacity can be measured using various biomarkers. Biomarkers such as ROS and SOD can serve as biological indicators for diagnosing OSA. In this study, the downregulated proteins primarily participate in oxygen transport, ROS metabolism and other related functions. These findings may be linked to oxidative stress induced by OSA, providing a novel venue for investigating childhood OSA.
We identified serum and urinary cathepsin Z and SHBG levels as being significantly associated with the duration of the medical history, and these levels gradually increased or decreased with the severity of OSA. Therefore, these proteins hold promise as potential biomarkers. We further conducted ELISA assays in a separate verification cohort and validated the proteomic findings and the significant differences between the control group and OSA of different magnitude. This observation suggests that the expression of cathepsin Z and SHBG may be linked to the progression of OSA.30 Current studies indicate that cathepsin Z is associated with the activity of immune cells such as neutrophils, macrophages, T cells and B cells.31 Single-cell analysis has also revealed specific expression of cathepsin Z in macrophages.29 Given the substantial activation of macrophages observed in children with OSA, this phenomenon may augment the inflammatory response. Notably, there is a lack of literature reports on the relationship between cathepsin Z and childhood OSA, and further inquiry on this issue may provide fresh perspectives for studying childhood OSA.32 SHBG, synthesized mainly by the liver, plays a crucial role in binding to circulating steroid hormones like testosterone and estradiol, thereby regulating their concentrations in the bloodstream. The serum level of SHBG is not only influenced by testosterone and estradiol but also affected by thyroid hormones and other metabolic factors. As a result, SHBG is considered as a potential biomarker for diseases such as33 type 2 diabetes,32 polycystic ovary syndrome and34 prostate cancer.35,36 Several reports have already shown lower expression levels of SHBG in OSA patients, which may be associated with reduced testosterone secretion in male patients.37 Some studies have also identified a close relationship between the decreased serum level of SHBG and the presence of circulating pro-inflammatory mediators. In this study, we observed a negative correlation between the expression levels of SHBG in the serum and urine of pediatric OSA patients and the severity of the disease. However, the specific mechanisms remain unclear. Therefore, further validation and understanding on the role of SHBG in pediatric OSA appear warranted.
In this study, a relatively high specificity and low sensitivity of cathepsin Z, SHBG or both proteins emerged when diagnosing pediatric OSA, showing that subjects predicted to have OSA did have OSA at the cost of missing some true OSA children. This prediction provides insight into the potential limitations of applying the aforementioned biomarkers and public health importance.
Our study has several limitations. First, the control group did not complete PSG because of the complexity of PSG and parental objection. However, we can essentially exclude that children in this group have OSA because no child showed symptoms of snoring, mouth breathing or enlarged tonsils, and their sleep-related breathing disorder scores were normal. Furthermore, all patients in this study were of East Asian descent, which may limit the evaluation of biomarker performance in other groups. Therefore, large-scale, multiethnic cohort studies are required to further validate the results. Second, we found a positive correlation between the expression of IGHG3, IGHG4, COMP and IGLV1-51 in both serum and urine with the severity of OSA. However, we were unable to validate these specific proteins because specific assays were not commercially available. Furthermore, technical limitations enabled only the validation of the expression of cathepsin Z and SHBG proteins in serum using ELISA. Therefore, as a next step, we plan to expand the sample size to further evaluate the sensitivity and specificity of cathepsin Z and SHBG expression in serum for diagnosing pediatric OSA. Finally, this was not an intervention study, and therefore we cannot infer causality regarding the putative biomarkers identified herein. Future studies aiming to overcome these limitations should provide greater insights into the pathogenesis of childhood OSA, and facilitate the diagnosis.
Two new biomarkers of pediatric OSA, namely cathepsin Z and SHBG, were identified using DIA MS. Both exhibit robust association with the severity of OSA and provide acceptable diagnostic capability. Thus, these biomarkers hold promise as valuable diagnostic and severity assessment tools for childhood OSA.
FundingThis study was supported by National Natural Science Foundation of China (82070092), Beijing Natural Science Foundation (7212033).
Contribution of each authorConceptualization: ZX, YZ, YW, ML, KZ. Investigation: YW, ML, KZ, JM, DG, ZX, YZ. Reporting: YW, ML, KZ, JM, DG, ZX, YZ. ZX is the guarantor of the paper, taking responsibility for the integrity of the work as a whole, from inception to published article.
Conflicts of interestThe authors declare no conflicts of interest related to this study.
Artificial intelligence involvementThe authors declare that there is no help of any artificial intelligence software or tools with this study.









