


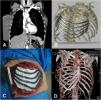
We present a 73 year-old woman with a history of breast prostheses, who had a tumor in her right breast. After removing the prosthesis in a private hospital, the tumor biopsy was reported as an undifferentiated pleomorphic sarcoma. The CT scan showed a large mass in the right breast involving the 4–8th ipsilateral ribs. After responding poorly to preoperative chemotherapy she was referred to our department, where we performed a 3D CT scan reconstruction to program the chest wall resection.1 We then worked with biomedical engineers to design a titanium dynamic prosthesis to cover the chest wall defect. The prosthesis is made of a Ti6Al4V which provides rigidity and lightness. It is designed with a tubular system that serves as a spring, allowing for mobility and ensuring proper fastening to the ribs without limiting respiratory movements. The surgery consisted of a bloc resection of the right breast and ipsilateral muscles involved (the pectoralis major, serratus major and partial latissimus dorsi). We then proceeded to the resection of the costal arches, from the 4th to the 8th to the sternal margin, and ligated the right internal mammary vessels. Next, we performed the reconstruction with a 3D dynamic prosthesis, which we fixed to the sternum with self-locking screws and cerclage to the ribs with a braided wire system (Dall-Miles). Due to the large size of the resection, we placed two Gore-Tex® mesh under the prosthesis and fastened them with non-absorbable monofilament loose stitches to protect the lung (Fig. 1).

In addition, a plastic surgeon proceeded to cover the prosthesis, checking the viability of the pedicle latissimus dorsi muscle, with ipsilateral translocation and advancement of the medial rest of pectoralis and the ipsilateral anterior rectum muscle.
The patient was discharged 10 days after the surgery, with good ventilatory mechanics, pain under control, and no respiratory complications. The histopathological result of the tumor was an undifferentiated pleomorphic sarcoma with free surgical resection margins without bone involvement. The CT scan showed the integration of the prosthesis in the chest wall like a native one, and the radioscopy images showed normal respiratory movements. Preoperative FEV1 1820mL (65%) compared with postoperative FEV1 after 6 months 1700mL (61%) in this case has shown non-differences in respiratory function tests.
A year and a half after the surgery, the patient shows no signs of recurrence in the CT scan follow-up, with no rupture, intolerance, or unanchoring of the prosthesis.
Surgical chest wall reconstruction is not standardized, and different materials were used in the past, such as synthetic meshes, biological meshes, rigid metal implants, etc.2 Ideally, the materials should be biocompatible without body rejection and promote bone tissue regeneration.
The use of dynamic prostheses designed with 3D printing technology allows for precise adaptability and adjustment to the anatomical wall defect needing repair.3–5 The design of the titanium prosthesis provides lightness while at the same time adequate rigidity, fulfilling the protective function of the internal organs. A titanium prosthesis consisting of articulated ribs is used, providing flexibility and preserving the patient's respiratory movements and functional capacity, so as to prevent possible postoperative respiratory complications associated with the static prostheses that were used previously. In our case, we chose 3D printed dynamic titanium prostheses for their lightness, hardness, and flexibility. In conclusion, we recommend the use of 3D dynamic prostheses in large chest wall resection involving the sternum or sternoclavicular joint.
FundingThis work has not received any funding.
Conflict of interestsThe authors state that they have no conflict of interests.







