




The knowledge of the relationship between exercise capacity and activities of daily living (ADLs) is important to minimize the negative outcomes in ADLs resulting from reduced exercise capacity in patients with chronic obstructive pulmonary disease (COPD). There is a limited study about the association between exercise capacity and ADLs in patients with COPD. This study aimed to investigate the relationship between maximal exercise capacity and ADLs in patients with GOLD stage II–III COPD.
MethodsTwenty-seven clinically stable GOLD stage II–III COPD patients were included (mean age=58.59±9.63 years and mean FEV1=50.6±13.7%) in this cross-sectional study. Maximal and submaximal exercise capacity were evaluated using an incremental shuttle walk test (ISWT) and 6-min walk test (6MWT), respectively. Activities of daily living were assessed using Glittre-ADL test.
ResultsThe ISWT distance was significantly correlated with Glittre-ADL test time (r=−0.517, p=0.006). There was also a negative correlation between 6MWT distance and Glittre-ADL test time (r=−0.506, p=0.007).
ConclusionA moderate relationship was found between maximal exercise capacity and general activities of daily living performance. The reduction in exercise capacity increases the negative influences in ADLs and strengthens our beliefs that exercise interventions in pulmonary rehabilitation could influence activities of daily living positively.
Es importante conocer la relación entre la capacidad de ejercicio y las actividades de la vida diaria (ADL) para minimizar los resultados negativos de las ADL que resultan de una capacidad reducida de ejercicio en pacientes con enfermedad pulmonar obstructiva crónica (EPOC). Los estudios sobre la asociación entre la capacidad de ejercicio y las ADL en pacientes con EPOC son limitados. En este estudio se investigó la relación entre la capacidad máxima de ejercicio y las ADL en pacientes con EPOC de estadios GOLD grado II-III.
MétodosEstudio transversal que incluyó a 27 pacientes clínicamente estables con EPOC de estadios GOLD grado II-III (edad media=58.59±9.63 años and FEV1 medio=50.6±13.7%). Las capacidades máxima y submáxima de ejercicio se evaluaron utilizando la prueba de lanzadera por tramos (ISWT) y la prueba de marcha de 6 minutos (6MWT) respectivamente. Las actividades de la vida diaria se evaluaron mediante el test de Glittre-ADL.
ResultadosLa distancia ISWT mostró una correlación significativa con el tiempo en el test Glittre-ADL (r=−0.517, p=0.006). También se observó una correlación negativa entre la distancia en el 6MWT y el tiempo en la prueba de Glittre-ADL (r=−0.506, p=0.007).
ConclusiónSe encontró una relación moderada entre la capacidad máxima de ejercicio y el desempeño general de las actividades de la vida diaria. La reducción en la capacidad de ejercicio aumenta las influencias negativas en las ADL y refuerza nuestras creencias de que las intervenciones con ejercicio tienen una influencia positiva en las actividades de la vida diaria en la rehabilitación pulmonar.
Chronic obstructive pulmonary disease (COPD), characterized by persistent and progressive airflow obstruction, is a chronic, preventable, and treatable disease. There are pulmonary and extrapulmonary components of impairments in COPD.1 Dyspnea and fatigue are the primary symptoms in patients with COPD arising due to the deteriorative effects of these components.1,2 Acute-on-chronic lung hyperinflation during exercise increases the mechanical loading of weak inspiratory muscles and inspiratory neural drive.3,4 Limitation of tidal volume increase as a result of decreased inspiratory capacity is primary reason for exertional dyspnea perception and exercise limitation.1,3,4
The activities of daily living (ADLs) are the involvement in activities on a daily basis. Whereas simple tasks such as mobility, drinking, eating, dressing, washing hands, and bathing can be described as basic ADLs, more complex tasks such as repairing a device, cutting fabric, ironing, managing finance, and home can be described as instrumental ADLs. The extrapulmonary effects of COPD may restrict the patients with COPD in maintaining their ADLs and their independence at home and/or outdoors.5 Lower extremity muscle strength was shown to be independent predictor of ADL performance in patients with COPD.6 Otherwise, aerobic exercise capacity must be sufficient to meet the increased oxygen demand to perform the simple ADLs.7 The patients with COPD experience higher metabolic load and symptom perceptions than healthy subjects during performing ADLs,8 and have limitations during ADLs. The most problematic ADLs were reported to be walking, household activities and stair climbing in moderate-very severe COPD.9
Although several studies investigated the relationship between submaximal exercise capacity and ADLs,10,11 there was any study investigating the relationship between maximal exercise capacity and ADL in patients with COPD. Accordingly, we aimed to investigate the relationship between maximal exercise capacity and ADLs with a performance based test in patients with GOLD stage II–III COPD. Our hypothesis was there was a more strong association between submaximal exercise capacity and ADL performance compared to maximal exercise capacity.
MethodsStudy designThis study was a cross-sectional study performed at the Department of Physiotherapy and Rehabilitation at Hacettepe University, Ankara, Turkey between 2013 January and December. The study was approved by Hacettepe University, Faculty of Medicine, Medical, Surgical and Drug Research Ethical Committee. The patients participating in the study signed the informed consent form explaining the scope and purpose of the study. This cross-sectional study was in agreement with the STROBE (Strengthening The Reporting of Observational Studies in Epidemiology) guidelines.
Study participantsTwenty-seven clinically stable GOLD stage II–III COPD patients with a mean age of 58.59±9.63 years were included. Patients who were referred to our department for the first time from Department of Chest Diseases at Hacettepe University and did not participate to a rehabilitation program before the study were included in the study when they meets the inclusion criteria in consecutive order. The flow diagram of the patient is presented in figure 1. Inclusion criteria was patients with GOLD stage II–III COPD who were not taking antibiotics and had not made any changes in their medications for at least three weeks. Patients with musculoskeletal and neurological disease, symptomatic heart disease, previous pulmonary surgery, malignant disease that may affect exercise performance, and patients who were unable to cooperate for measurements and evaluations were excluded. G*Power program version 3.1 (Universität Düsseldorf, Düsseldorf, Germany) was used to calculate the sample size. The purpose of the study was to determine the correlation between ISWT distance and Glittre ADL test duration. The aim to get significant results (p<0.05) with sufficient power (80%) to detect was at least correlation coefficient 0.5. Therefore, the minimum required sample size for the study was 26. The formula for calculation is based on two-tailed calculations.12
Study procedure
Anthropometric features such as age, gender, height, and body weight were recorded.
Dyspnea perceptions during daily life was recorded according to the modified Medical Research Council dyspnea scale (MMRC) score.13 Patients underwent pulmonary function test using the spirometer (Spirolab, Medical International Research, Rome, Italy) based on the recommendations of the American Thoracic Society (ATS)/the European Respiratory Society (ERS).14
The patients performed an incremental shuttle walk test (ISWT) and 6-min walk test (6MWT) for the assessment of maximal and submaximal exercise capacity, respectively. The ISWT is an externally paced, maximal exercise test. Pre-recorded signals control the speed of walking. The walking speed increases until the participant can no longer continue. For ISWT, two cones with a distance of 9m were used. Rotations around the cones are accepted as 0.5m, and each shuttle was accepted as 10m. The participants were asked to walk at an increasing rate between the two cones adapting their walking speed according to the signals.15 The completed distances of the participants were recorded both as meters and a percentage of predicted distance was calculated according to reference equations.16
The 6MWT, a self-paced and submaximal test, measures the distance that a patient can walk on a flat corridor for six minutes. During the 6MWT, participants were asked to walk as fast as they could in a 30-m straight corridor with their walking tempo for six minutes with standardized encouragements.15 The completed distances of the participants were recorded both as meters and a percentage of predicted distance was calculated according to reference equations.17
The ADL performance was assessed with Glittre-ADL test. The activities in the Glittre-ADL test were chosen to represent activities commonly required for everyday life and known to be distressing for COPD.18 The test begins while the patient is in the sitting position. The patient then passes over the two-step ladder placed in the middle, walking to the two shelves set according to the patients’ shoulder and waistline. The three bottles weighing 1kg is carried from the top shelf to the lowest shelf, and then finally to the top shelf. The patient then turns, goes back to the chair and sits down, gets up quickly and starts the other round. The test has five rounds and patients are asked to complete these rounds as quickly as possible. They are allowed to rest if necessary but are asked to return to the action as soon as possible. During the test, female patients carry 2.5kg, and male patients carry 5kg backpack. Each step of the ladders’ height and width are 17cm and 27cm, respectively. Duration of the test was recorded as minutes.18
Statistical methodsThe data were analyzed using the Statistical Package for the Social Sciences version 20.0 (IBM, Armonk, NY, USA).19 Descriptive statistics were used to exhibit participant characteristics. Data were expressed as the mean±standard deviation unless stated otherwise. All variables were tested using visual (histograms/probability plots) and Shapiro–Wilk test for normality. Spearman's rank correlation coefficients were used to assess the relationships between maximal exercise capacity and daily living activities.20 Correlations were classed as “strong” (r>0.70), “moderate” (r=0.50–0.69), “weak” (r=0.26–0.49), and “very weak or no correlation” (r=0.00–0.25).21 A p value <0.05 was considered statistically significant.20
ResultsThe characteristics of 27 patients with COPD were shown in Table 1. Thirteen of COPD patients (48.1%) had moderate severity COPD (GOLD stage II), 14 of them (51.9%) had severe COPD (GOLD stage III). Twenty-one of the patients (77.8%) were ex-smokers, six of them (22.2%) were never smoked. Median MMRC score of COPD patients was 2.
Patients’ characteristics (n=27).
| Variable | Mean±SD | Range |
|---|---|---|
| Age (years) | 58.59±9.63 | 41–74 |
| Sex (female/male) | 9/18 | |
| Weight (kg) | 73.42±11.26 | 45–95 |
| Height (cm) | 165.88±8.85 | 147–180 |
| BMI (kg/m2) | 26.79±4.39 | 16.28–33–87 |
| Cigarette smoking (pack-years) | 33.64±29.41 | 0–100 |
| MMRC score (0–4) | 2 | 0–3 |
| Pulmonary function test | ||
| FEV1 (L) | 1.45±0.49 | 0.75–2.61 |
| FEV (predicted %) | 50.59±13.72 | 28.00–85.00 |
| FVC (L) | 2.36±0.77 | 0.89–3.87 |
| FVC (predicted %) | 66.25±15.00 | 37.00–106.00 |
| FEV1/FVC (%) | 63.88±17.13 | 30.10–94.40 |
| FEF25–75% (L) | 1.12±0.70 | 0.29–2.91 |
| FEF25–75% (predicted %) | 33.46±18.13 | 9.00–89.00 |
| PEF (L) | 3.96±1.46 | 1.50–6.52 |
| PEF (predicted %) | 52.66±18.59 | 22.90–92.00 |
BMI: body mass index; MMRC: the modified Medical Research Council dyspnea scale; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; FEF25–75%: 25% and 75% of the forced vital capacity; PEF: peak expiratory flow.
Data on the patients’ outcomes of Glittre ADL test, ISWT, and 6MWT are demonstrated in Table 2. The reasons for termination of the ISWT were as mainly because the patients were not as fast as to reach the signals’ speed. Twelve of the patients (44.4%) missed two cones. The mean distance of ISWT was 382.59±152.83m, and the mean percentage of the predicted ISWT distance was 50.31±16.80%. The mean distance of 6MWT was 488.26±96.80m. The mean percentage of predicted 6MWT distance was 98.40±20.50%.
Patients’ outcomes of Glittre activities of daily living test, incremental shuttle walk test, and 6-min walk test.
| Parameters | Glittre-ADL | ISWT | 6MWT |
|---|---|---|---|
| Mean±SD | Mean±SD | Mean±SD | |
| HR (beats/min) | |||
| Pre-test | 83.92±9.52 | 85.70±9.92 | 81.59±13.30 |
| Post-test | 114.96±19.90 | 130.07±17.76 | 112.70±23.66 |
| SpO2(%) | |||
| Pre-test | 95.77±1.90 | 94.22±3.94 | 95.14±2.94 |
| Post-test | 91.00±5.36 | 90.03±5.80 | 92.18±5.15 |
| Dyspnea (Borg scale) | |||
| Pre-test | 0.74±0.92 | 0.61±0.96 | 0.64±0.97 |
| Post-test | 4.88±2.69 | 5.03±2.80 | 3.42±2.31 |
| Arm fatigue (Borg scale) | |||
| Pre-test | 0.98±1.20 | NA | NA |
| Post-test | 2.55±2.25 | ||
| Leg fatigue (Borg scale) | |||
| Pre-test | 0.68±1.01 | 0.38±0.72 | 0.55±1.03 |
| Post-test | 3.00±2.48 | 4.25±2.82 | 2.68±2.59 |
| General fatigue (Borg scale) | |||
| Pre-test | 1.25±1.33 | 1.03±1.20 | |
| Post-test | 3.77±2.53 | 3.07±2.50 | |
| Test time (min) | 2.87±1.22 | NA | NA |
| Distance (m) | NA | 382.59±152.83 | 488.26±96.80 |
HR: heart rate; SpO2: oxygen saturation; ADL: activities of daily living; ISWT: incremental shuttle walk test; 6MWT: 6-min walk test; NA: not applicable.
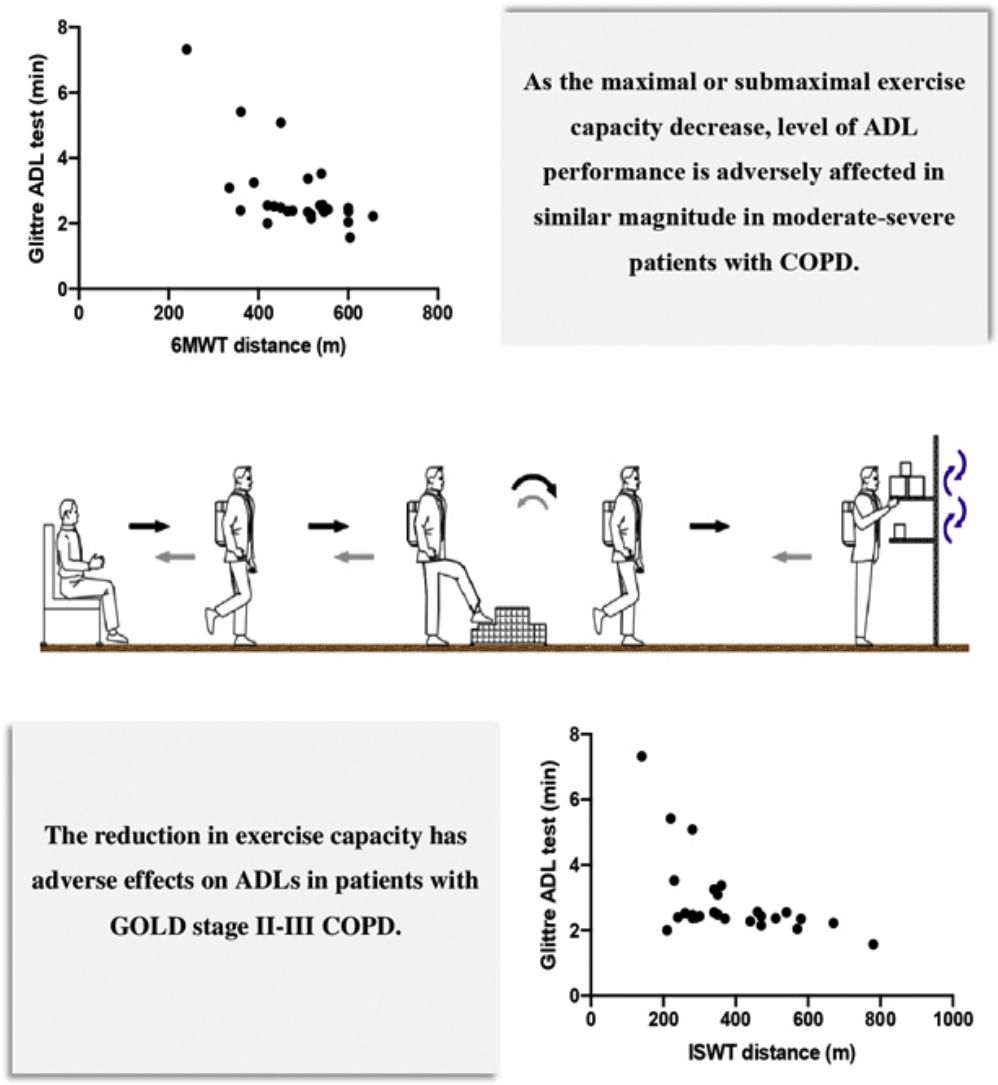
There was a negative correlation between 6MWT distance and Glittre-ADL test time (r=−0.506, p=0.007, Fig. 2). The ISWT distance was significantly correlated with Glittre-ADL test time (r=−0.517, p=0.006, Fig. 3). In addition, the MMRC dyspnea score was significantly correlated with 6MWT distance (r=−0.535, p=0.004) and the ISWT distance (r=−0.417, p=0.031). Although there was any correlation between MMRC dyspnea score and Glittre-ADL test time (p>0.05), MMRC dyspnea score was weakly associated with the increase in dyspnea perception during ADL (r=0.423, p=0.028).
.")
.")
When we look at the correlations between symptom perceptions during exercise tests and ADL performance, increase in dyspnea perception during 6MWT was moderately associated with the increase in dyspnea perception during ADL (r=0.667, p<0.001). The leg fatigue perception increase in 6MWT was moderately correlated with the increase in leg fatigue perception during ADL (r=0.498, p=0.008). The change in SpO2 during 6MWT was moderately associated with the change in SpO2 during ADL (r=0.608, p=0.001). The increase in HR during 6MWT was correlated with the increase in HR during ADL (r=0.568, p=0.002). Otherwise, the change in SpO2 during ISWT was moderately associated with the change in SpO2 during ADL (r=0.620, p=0.001). The leg fatigue perception increase in ISWT was moderately correlated with the increase in leg fatigue perception during ADL (r=0.592, p=0.002) and also arm fatigue increase during ADL (r=0.524, p=0.005).
DiscussionThis study revealed that as the maximal or submaximal exercise capacity decrease, level of ADL performance is adversely affected in similar magnitude in moderate–severe patients with COPD. In addition, dyspnea perception level in daily life is related with increased dyspnea perception in ADL performance and decreased exercise capacity. Otherwise, only dyspnea perception increase during submaximal exercise is related with increase in dyspnea during ADL performance.
Shouza et al. showed that although there was any difference between Glittre-ADL test times between GOLD 1–3 COPD patients, as the disease severity progresses, the ratio of Glittre-ADL oxygen consumption (VO2)/peak VO2 during cardiopulmonary exercise testing (CPET) increased significantly. In addition, the severe COPD patients presented lower ventilator and cardiac reserve, higher dyspnea perception and SpO2 decline at the end of the Glittre-ADL test.22 Vaes et al. reported that patients with COPD used a significantly higher proportion of their peak exercise capacity and ventilation than healthy controls during five specific ADLs, which are putting on socks, shoes, and vest; folding eight towels; putting away groceries; washing four dishes, cups, and saucers; and sweeping the floor for four minutes.8 Different studies are supporting the evidence that VO2 and ventilatory demand were higher in patients with COPD than in healthy controls during daily activities.23,24 Our patients had reduced maximal exercise capacity (50.31±16.80%) and this reduction was correlated with the poor ADL performance. Although we were unable to assess the oxygen uptake during activities of the patients in our study, ISWT distance and peak oxygen uptake have similar accuracy for the estimation of peak exercise capacity in patients with COPD.25 These result supports the findings that reduced ventilator and metabolic reserve during exercise are reflected in daily life that contains movements of upper and lower extremities.8,22 Otherwise, the deoxygenation and increased leg fatigue perceptions during ISWT was associated with deoxygenation and increased leg and arm fatigue perceptions during ADL performance. These findings demonstrates us that ADL performance is negatively affected and level of deoxygenation and fatigue perceptions increases during daily activities as a result of diminished ventilator reserve during exercise in COPD patients.4 In line with these results, dyspnea perception during life that was evaluated by MMRC score was correlated with ISWT distance. A recently published study in 2018 suggested that phases of desaturation (especially <88%) during laboratory based ADL test is correlated with desaturation phases during daily life.26 In accordance with these results, change in oxygenation level was correlated between ISWT and Glittre-ADL test. Therefore, the ISWT as a field test, may be a practical alternative to estimate the ADL performance in patients with COPD when oxygen uptake cannot be measured in the clinical settings.
In a study investigating the relationship between functional performance and Glittre-ADL test, Glittre-ADL test time of GOLD II and GOLD III COPD patients was reported to be 4.02 and 4.87min, respectively.27 Gulart et al. reported that the mean Glittre-ADL test time was 4.63±1.95min, the 6MWT distance was 424±1.60m in their study of approximately 62% GOLD II–III COPD patients of the participants.28 In the present study, Glittre-ADL test time was lower, and 6MWT distance was longer compared to the previous studies.27,28 This difference may be a result of different patient characteristics such as lower mean age, lower body mass index, higher FEV1 values, and mostly male gender in the present study.
Ozsoy et al. showed that London Chest ADL score (LCADL) that is a paper-based ADL questionnaire is correlated with 6MWT distance (r=−0.48, p=0.001) and functional exercise capacity, symptom perceptions increase and expiratory muscle strength are predictors of ADL in COPD.11 Another study demonstrated that the Glittre-ADL test performance is related with the walking and sitting time during daily life.27 The Glittre-ADL test performance was also associated with the daily physical activities (r=0.67, p<0.05) and with 6MWT distance (r=−0.64, p<0.05) in a trial by Correa et al. in 2011.10 Our study was in agreement with previous findings that submaximal exercise capacity is more closely associated with ADLs and more reflects the influence on ADLs.10,11,27 The COPD Assessment Test that evaluates impact of disease on functional status and symptom perceptions (cough, phlegm, chest tightness, dyspnea, activities, confidence, sleep, and energy) was shown to be related with 6MWT distance, performance based Glittre-ADL test time and LCADL score.28 We also demonstrated that dyspnea and leg fatigue perceptions, oxygenation level and HR increase during 6MWT and Glittre-ADL test was similar. Also the MMRC score was correlated with dyspnea increase in ADL. This supports that 6MWT and Glittre-ADL test are two important functional tests that can reflect daily living activities. The other reason for the symptom perceptions and changes in HR and SpO2 at same amount during both tests are that they are submaximal tests.
Some limitations of this study have to be made clear. First of all, we did not include a control group. Secondly, we were unable to measure the oxygen consumption during Glittre-ADL test, ISWT, and 6MWT due to the laboratory facilities. Measuring oxygen consumption during ADL and field tests may provide the determination of the ventilatory limitation and metabolic cost of these activities and enable the comparison of these outcomes among different tests such as Glittre-ADL test, 6MWT, and ISWT. Additionally, we did not include mild and very severe patient group. Therefore, this can limit the generalizability of the outcome of the study.
ConclusionsIn conclusion, the reduction in exercise capacity has adverse effects on ADLs in patients with GOLD stage II–III COPD. In addition, increase dyspnea perception cause decline in maximal and submaximal exercise capacity and symptom perception increase during exercise is related with symptom perception increase during ADLs. These results strengthen the necessity of exercise interventions in order to reverse the unfavorable outcomes in the ADLs resulting from reduced exercise capacity. To our knowledge, there is limited data about the relationship between maximal exercise capacity and daily living activities in literature and present study is the important for investigating this topic. Further randomized controlled studies with larger sample size and COPD patients from all stages are needed that evaluates maximal exercise capacity and activities of daily living relation. There is also need for researches that investigate the effects of exercise training on ADLs.
Conflict of interestsThe authors declare no conflict of interests.
This study was presented during a poster session at the European Respiratory Society International Congress, September 15–19, 2018, in Paris, France.







