Non-invasive ventilation (NIV) is used in the management of acute respiratory failure to alleviate the work of breathing, primarily performed by the diaphragm. Assessing diaphragmatic function under NIV is a challenging task, especially distinguishing between the muscle's autonomous effort and the support provided by the ventilator. But it is highly relevant, since it is necessary to set the ventilators matching the patients’ needs, avoiding over and under assistance.3 In absence of objective measurements, physicians may use clinical and physical observations at the patients’ bedside subjected to a great interobserver variability.
One way to assess the diaphragmatic function non-invasively is by measuring its excursion movement1 using ultrasound. This method has been validated2 in spontaneously breathing patients, but not in those receiving MV, as it is impossible to separate the autonomous displacement of the diaphragm from the one generated by the ventilator. Then another tool has been proposed: the diaphragmatic shortening fraction.3 It focuses in the changes of the diaphragm thickness in the apposition zone during active inspiration. Although it is not interfered by the pressure delivered from the ventilator, it is a laborious, poorly reproducible technique, not easy to perform in acute scenarios.4 Other ways to monitoring diaphragmatic effort include electromyography or transdiaphragmatic pressure, being those methods invasive, difficult to perform and expensive approaches.
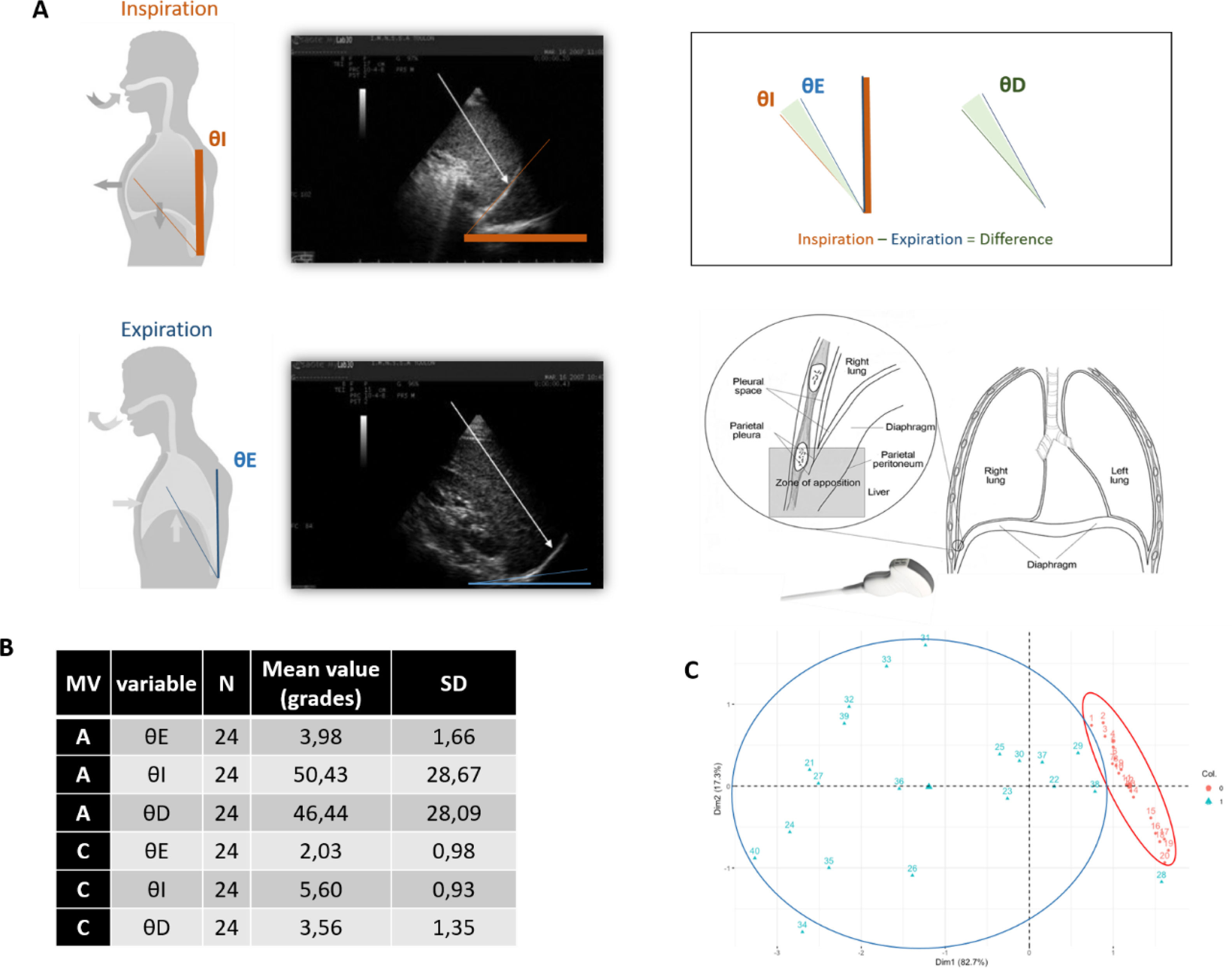
We propose a novel method to estimate diaphragmatic activity using ultrasound by measuring the theta (θ) angle, visible at the diaphragm's apposition region, hypothesizing that changes in this angle can reflect the degree of diaphragmatic effort (Fig. 1).
 Graphic representation of θ angle and its acquision. Different phases: inspiratory (θI), expiratory (θE) and the difference between them (θD). (B) Main data: Mean measures for each phase of the angle and standard deviation of data collected in assisted (A) and controlled cycles (C). We recorded 3 times each angle for each patient (N=8) MV (mechanical ventilation) SD (standard deviation). (C) Principal Component Analysis (PCA). The data of all the variables are grouped into small values in a situation of CMV and large values in AMV. D=1, p-value=4.122e−09.")
(A) Graphic representation of θ angle and its acquision. Different phases: inspiratory (θI), expiratory (θE) and the difference between them (θD). (B) Main data: Mean measures for each phase of the angle and standard deviation of data collected in assisted (A) and controlled cycles (C). We recorded 3 times each angle for each patient (N=8) MV (mechanical ventilation) SD (standard deviation). (C) Principal Component Analysis (PCA). The data of all the variables are grouped into small values in a situation of CMV and large values in AMV. D=1, p-value=4.122e−09.
The θ angle is defined by two lines: one along the patient's spine and another tangential to the diaphragmatic dome. Measurements taken during inspiratory (θI), and expiratory phases (θE), in order to calculate the difference between these angles (θD) We hypothesize that θD must be the most accurate measure, since θD subtracts from the contraction angle θI the extra degrees that the positive pressure of the respirator could provide, registered as θE.
To test this, we recorded θ angle measurements during assisted and controlled mechanical ventilation (ACV and CMV respectively) cycles in the same patients, for three times each. Given that CMV involves passive insufflation, we expected higher θD values during AMV, reflecting the effort required to trigger the ventilator.
We selected consecutive and stable patients from our Intermediate Respiratory Care Unit (IRCU) who required NIV to perform the measurements. All patients were ventilated with a Phillips® V60 ventilator in S/T mode, with IPAP 18mmHg and EPAP 8mmHg. Triggers were driven by Autotrack® system. The back-up respiratory rate was 14 respirations per minute. The inspiratory time (Ti) was adjusted to neuromechanical Ti. With this set up, patients had to maintain a 8±2L/min minute ventilation. Exclusion criteria included any kind of encephalopathy, poor consciousness level, known diaphragmatic dysfunction and the use of sedative drugs.
Eight patients met the inclusion criteria and successfully transitioned CMV during the trial. We used a VenueGo GE® echograph with a convex probe. All the measurements were made by a single physician with the ecograph's software.
Several analyses were performed. With K-means cluster analysis it is easy to see how the data related to poor diaphragmatic effort are in the vicinity of CMV and the opposite occurs in AMV (Fig. 2). In the PCA (Principal Component Analysis) the data of all the variables are grouped into small values in a situation of CMV and large values in AMV. A distribution was made in 2 dimensions D=1, p-value<0.05, being significant (Fig. 1).
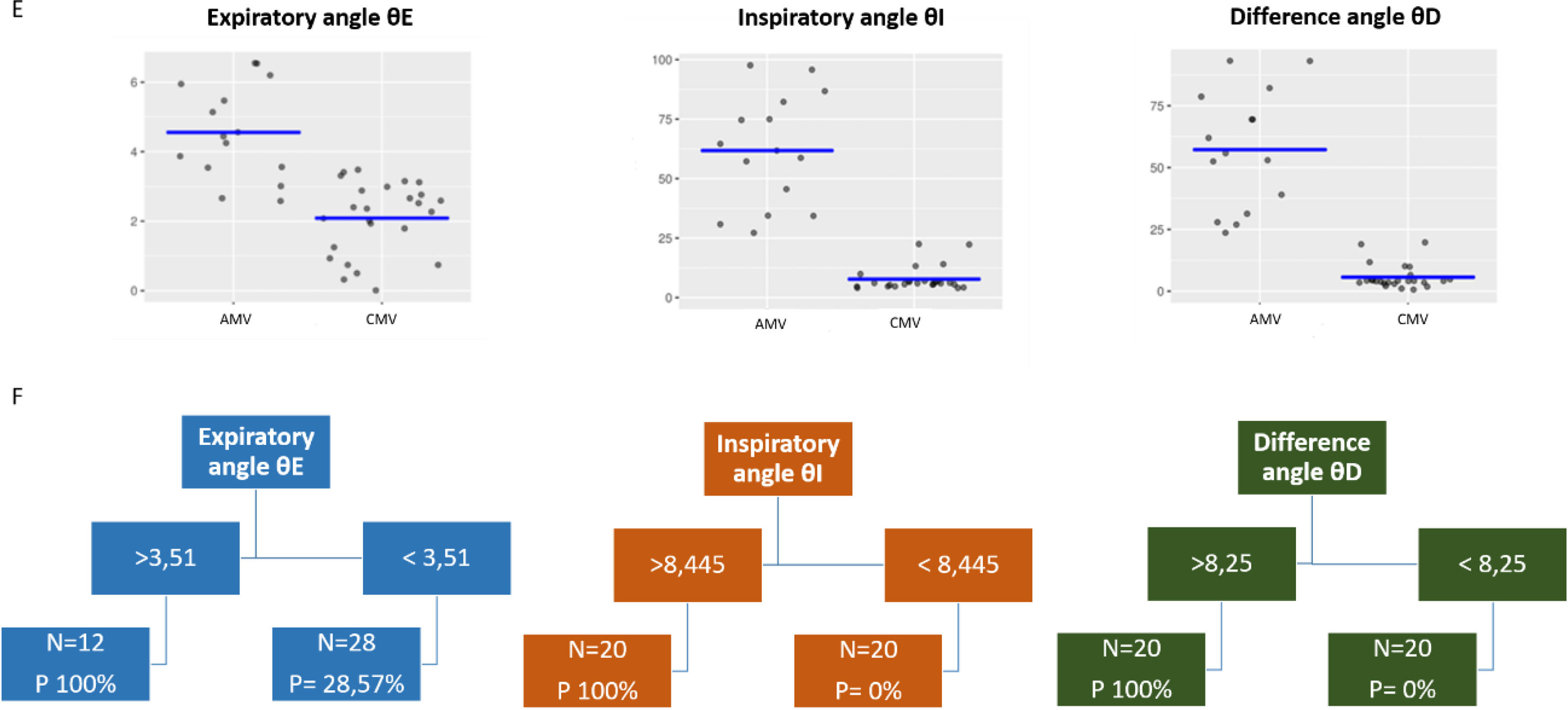
 K means cluster analysis, visual representation parallel coordinates plot of the distribution of variables in AMV and CMV. Percentage of within cluster heterogeneity accounted for by each cluster: Cluster 1: 50.83%, Cluster 2: 49.17%. Between cluster heterogeneity accounts for 65.82% of the total heterogeneity in the data (higher is better). (F) Classification tree, cut-off points of each variable. The cycle was predictably AMV when the θD was ≥to 8.25 θI was ≥to 8.445 and the θE was ≥to 3.51.")
(E) K means cluster analysis, visual representation parallel coordinates plot of the distribution of variables in AMV and CMV. Percentage of within cluster heterogeneity accounted for by each cluster: Cluster 1: 50.83%, Cluster 2: 49.17%. Between cluster heterogeneity accounts for 65.82% of the total heterogeneity in the data (higher is better). (F) Classification tree, cut-off points of each variable. The cycle was predictably AMV when the θD was ≥to 8.25 θI was ≥to 8.445 and the θE was ≥to 3.51.
Using binary Logistic Regression Analysis, we saw that θD was the variable that best discriminates between the classes (active or passive cycling, that is AMV or CMV) with an Odds ratio 3.366, (lower limit 1.711, upper limit 9.504 and a p-value<0.05. The ROC curve) established considering potential bias due to the use of repeated data showed an AUC for a 95% confidence interval of 0.83 (0.7–0.96).
The cut-off points of each variable were deduced from classification tree analysis. The cycle was predictably AMV when the θD was ≥to 8.25, θI was ≥to 8.445 and the θE was ≥to 3.51. The most important variables selected in the model were the θD and θI. At the same time the sub analysis of partial dependence indicates that the single analysis of θI would be enough to execute the θ angle method accurately (Fig. 2).
A Random Forest Analysis yielded an R-squared of 0.925 with a prediction error of 0.138 overall. The ROC curve was analyzed separately with the predictive statistics of the θD (R-squared 0.99 and prediction error<0.051), θI (R-squared 0.89 and error prediction<0.162) and θE (R-squared 0.011 and prediction error<0.504), being the latter suboptimal for the model.
The results suggest that θ angle, specially θD, is a promising tool for assessing diaphragmatic effort in patients under MV. The use of ultrasound could avoid the use of expensive, invasive, difficult to perform techniques to detect effort and maybe, quantified it. In this line, as part of our investigation, we compared θD with the electrical activity of NAVA (EADi) in a subject undergoing invasive mechanical ventilation, during a sedation window. Linear regression equations were carried out between NAVA electrical activity and θD with the equation y=8.258x+18.513 and R2=0.9567. Paired t-test data for the relation between NAVA and θD was t=−15.034, dif=11, p-value=1. Therefore, both methods seem to correlate when measuring the magnitude of respiratory effort, though this observation needs further investigation.
Our study has limitations, including a small, heterogeneous sample size. Additionally, the reproducibility of the technique needs further validation. Future studies should correlate our measurements with transdiaphragmatic pressure, the gold standard for measuring diaphragmatic effort.
Finally, our results suggest that ultrasound can be used to predict diaphragmatic activation and detect and maybe quantify effort in patients under NIV by measuring the θD angle, which represents a simple, noninvasive, and suitable method. Analyzing all our tests, for an easier approach, probably θI is reliable as well and faster to acquired. These tools could allow physicians to adjust the parameters of a ventilator to minimize the objective respiratory effort. This is a relevant leap that can change our actual clinical practice towards a more personalized and safer one.
Conflict of InterestsThe authors state that they have no conflict of interests.







