







Muscle mass maybe a determining factor in the variability of spirometry results in individuals of the same sex and age who have similar anthropometric characteristics. The aim of this study was to determine the association between spirometric results from healthy individuals and their muscle mass assessed by dual energy X-ray absorptiometry (DEXA).
MethodsA sample of 161 women and 144 men, all healthy non-smokers, was studied. Ages ranged from18 to77years. For each subject, spirometry results and total and regional lean mass values obtained by full body DEXA were recorded. A descriptive analysis of the variables and a regression analysis were performed to study the relationship between spirometric variables and lean body mass, correcting for age and body mass index (BMI).
ResultsIn both sexes all muscle mass variables correlated positively and significantly with spirometric variables, and to a greater extent in men. After partial adjustment of correlations by age and BMI, the factor which best explains the spirometric variables is the total lean body mass in men, and trunk lean body mass in women.
ConclusionsIn men, muscle mass in the lower extremities is most closely associated with spirometric results. In women, it is the muscle mass of the trunk. In both sexes muscle mass mainly affects FEV1.
La cantidad de masa muscular podría ser un factor determinante que explicara la variabilidad de los resultados de la espirometría en individuos del mismo sexo y edad y de características antropométricas similares. El objetivo de este estudio es determinar si existe asociación entre los resultados espirométricos de individuos sanos y su masa muscular estimada mediante absorciometría de rayos X (DEXA).
MétodosSe estudió una muestra de 161 mujeres y 143 varones sanos, no fumadores, de 18 a 77años. En cada sujeto se registraron los resultados de una espirometría y los valores de la masa magra total y regional obtenidos mediante DEXA. Se realizó un análisis descriptivo de las variables y un análisis de regresión para estudiar las relaciones entre variables espirométricas y masa magra, corrigiendo los efectos que pudieran ejercer la edad y el índice de masa corporal (IMC).
ResultadosEn ambos sexos todas las variables de masa magra se correlacionan de forma positiva y significativa con las variables espirométricas, siendo estas relaciones mayores en los varones. Al ajustar estas correlaciones de forma parcial por la edad y el IMC, lo que mejor explica las variables espirométricas es la masa magra en las extremidades inferiores en varones, y la masa magra del tronco en mujeres.
ConclusionesEn los varones, la masa muscular en las extremidades inferiores es la que más se asocia a los resultados espirométricos. En las mujeres es la masa muscular del tronco. En ambos sexos la masa muscular influye principalmente sobre el volumen espiratorio forzado en el primer segundo (FEV1).
Forced spirometry is the principal test for evaluating lung function in individuals. The main factors determining spirometric results are sex, age, height, and weight, and these variables are used to produce equations predicting normal reference values. Several authors1,2 believe that there must be other factors that determine spirometry results, which would explain the variability in test values obtained in healthy individuals with similar characteristics. The premise of this study is that one of the factors that might cause this variability could be muscle mass. Although some previous studies3–6 have already evaluated this possibility, we believe that the influence of an individual's muscle mass on spirometric results has not been clearly established.
The technique of choice for evaluating muscle mass is dual energy X-ray absorptiometry (DEXA). This is an imaging technique used to quantify lean body mass (fat-free mass) in both the whole body and in different body regions. Lean body mass is an estimation of muscle mass. This test offers reliable measurements that are comparable over time. It is, moreover, a technique widely used in respiratory clinics,7–9 mainly for assessing muscle mass in patients with chronic obstructive pulmonary disease (COPD), who often present muscle dysfunction of the ventilatory system and the lower limbs.10,11 Muscle training improves exercise tolerance, muscle strength, dyspnea, fatigue, and quality of life in these patients. The impact of muscle mass on the symptoms and prognosis of asthmatics has also been studied.12,13 Increasing numbers of studies are using DEXA to evaluate the outcome of muscle training in respiratory rehabilitation programs in COPD patients and to determine their prognosis.14–17 For this reason, we identified a need to establish the association between spirometric values and muscle mass parameters determined by DEXA in healthy individuals.
The aim of this study was to quantify the association between spirometric variables and muscle mass estimated by DEXA, to establish whether muscle mass is an important determinant in the spirometric results of healthy individuals, and to help establish the normality of this association.
MethodsStudy SubjectsThe study population consisted of 305 healthy subjects of Caucasian origin (144 men and 161 women), aged between 18 and 77 years, inclusive. Participation in the study was voluntary, and all subjects were recruited from an urban setting in the environs of the Universidad de Alcalá de Henares. Subjects were matched in terms of lifestyle and diet, and had performed physical exercise sporadically throughout their lives.
Study inclusion criteria were:
- -
Never-smoker.
- -
No metabolic diseases or pharmacological treatments that might alter metabolism.
- -
No muscle or neuromuscular diseases.
- -
No thoracic abnormalities, determined as a thoracic index within the mean for their age, plus or minus 2 standard deviations.
- -
No obvious changes in the physiological curvature of the spine.
- -
No neoplasms, cardiovascular diseases, chronic bronchial diseases, or episodes of spontaneous pneumothorax.
All individuals had spirometric results within normal limits (forced vital capacity [FVC] and forced expiratory volume in 1s [FEV1] over 80% predicted, and FEV1/FVC greater than 70% and less than 80%), and agreed voluntarily to undergo the specific study tests, after giving informed consent.
MethodsMuscle Mass AssessmentTo quantify muscle mass in each individual, a whole-body dual energy X-ray absorptiometry (DEXA) was performed, from which overall and regional lean body mass (fat-free soft tissue mass) values were obtained, providing an estimation of muscle mass.
This technique uses a highly stable X-ray generator to produce a spectrum of broad energy band levels. The apparatus consists of NaI crystal scintillation detectors placed in tandem. The source of radiation and the detectors are placed opposite each other and mechanically connected so that they move simultaneously. The light beam passes in a posteroanterior direction through the tissue while the patient lies perfectly still in a supine position. Energy is absorbed depending on the density of the tissue that it passes through: absorption is zero in air, small in fat, greater in soft tissues, and very significant in bone. Photons that have not been absorbed are captured by the detector, so the density of the area explored is proportional to the attenuation of radiation by the tissue.
This is a safe technique, since the dose of radiation used is minimal, and very little inter and intra-observer variation has been demonstrated, making it very useful for research.
In our study, we quantified, in grams:
- -
Total lean mass (TLM).
- -
Trunk lean mass (TrLM).
- -
Leg lean mass (LLM).
The examination was performed using the Norland densitometer XR-800 TM WITH Illuminatus software version 4.5.0 (Norland, a CooperSurgical Company, Fort Atkinson, WI, U.S.). All densitometries were performed following standardized protocols provided by the manufacturer and described by Aguado et al.18
All examinations were performed using the same equipment, in the same laboratory by the same technician.
Evaluation of Lung FunctionAll subjects underwent forced spirometry with a COSMED K4 b2 turbine spirometer, after calibration of the flow measured using a calibration syringe certified by the American Thoracic Society (ATS). The spirometry study was performed according to the protocol recommended by the Spanish Society of Pulmonology and Thoracic Surgery (SEPAR).19 Absolute FVC and FEV1 values were measured in milliliters (ml), and peak expiratory flow (PEF) and forced expiratory flow between 25% and 75% of forced vital capacity (FEF25%–75%) were measured in liters per second.
All tests were performed by the same technician, in the same laboratory, using the same equipment.
AnalysisThe statistical analysis was performed using the SPSS 22.0 and Statgraphics Centurion 17 package for Windows.
The arithmetic mean, standard deviation, and minimum and maximum values were obtained for men and women. Differences in means of both sexes were evaluated using the t test for independent samples.
To explore linear associations between the spirometric variables and the lean mass variables, principal components analysis on the correlation matrix was used to reduce dimensionality, obtaining a 2-dimensional graphic that revealed the relationships between the variables, so that the more acute the angle formed, the greater the linear relationship.
Relationships between the different spirometric variables and the lean mass variables were analyzed using correlations. Partial correlations were used, adjusting for age and body mass index (BMI), to eliminate the possible effect of confounding factors (age, height and weight).
A multiple linear regression analysis was performed to determine if the lean mass variables could be considered as predictive factor for spirometric variables.
ResultsDescriptive statistics of the muscle mass and lung function variables in men and women are shown in Table 1.
Descriptive Statistics of Study Participants.
| Women | Men | p | |
|---|---|---|---|
| Mean, Standard Deviation, and Range | Mean, Standard Deviation, and Range | ||
| Age (years) | 46.4±16.8 (18–75) | 43.3±16.7 (18–77) | |
| Height (cm) | 159.9±7 (143–185) | 173.2±7.5 (154–190) | ** |
| Weight (kg) | 63.8±10.1 (44–97) | 80.9±12.4 (60–119) | ** |
| BMI | 25±4.3 (16.6–41.9) | 26.9±3.8 (19.7–40.8) | |
| FVC (ml) | 3334.2±691.5 (1370–4720) | 4711.5±848.3 (2610–7000) | ** |
| FEV1 (ml) | 2830.3±614.7 (1150–4060) | 3855.9±785.3 (1890–5920) | ** |
| PEF | 6212.1±1407.9 (2380–10390) | 9066.1±1959.7 (3170–1.3270) | ** |
| FEF25%–75% | 3226.8±943.6 (1040–6530) | 3985.7±1315.6 (1340–8660) | ** |
| FEV1/FVC | 84±5.8 (70–99) | 82±5.8 (71–95) | |
| TLM (kg) | 34.9±44.9 (23.1–49.8) | 55.2±75.1 (40.6–77.2) | ** |
| TrLM (kg) | 15.5±22.1 (10.5–23.2) | 25.2±38.8 (12.2–38.1) | ** |
| LLM (kg) | 12.7±19.8 (7.7–18.8) | 19.3±30 (13.9–27.3) | ** |
FEF25%–75%: midexpiratory flow; FEV1: forced expiratory volume in 1s; FVC: forced vital capacity; PEF: peak expiratory flow; LLM: leg lean mass; TLM: total lean body mass; TrLM: trunk lean mass.
All variables analyzed showed significant differences in mean values of both sexes, except age and sex. Means were higher in men, as shown in Table 1, with statistically significant p values.
In the principal components analysis, positive correlations between all spirometric variables and all lean mass variables were found in both sexes, with the greatest correlation being observed for LLM (Figs. 1 and 2).
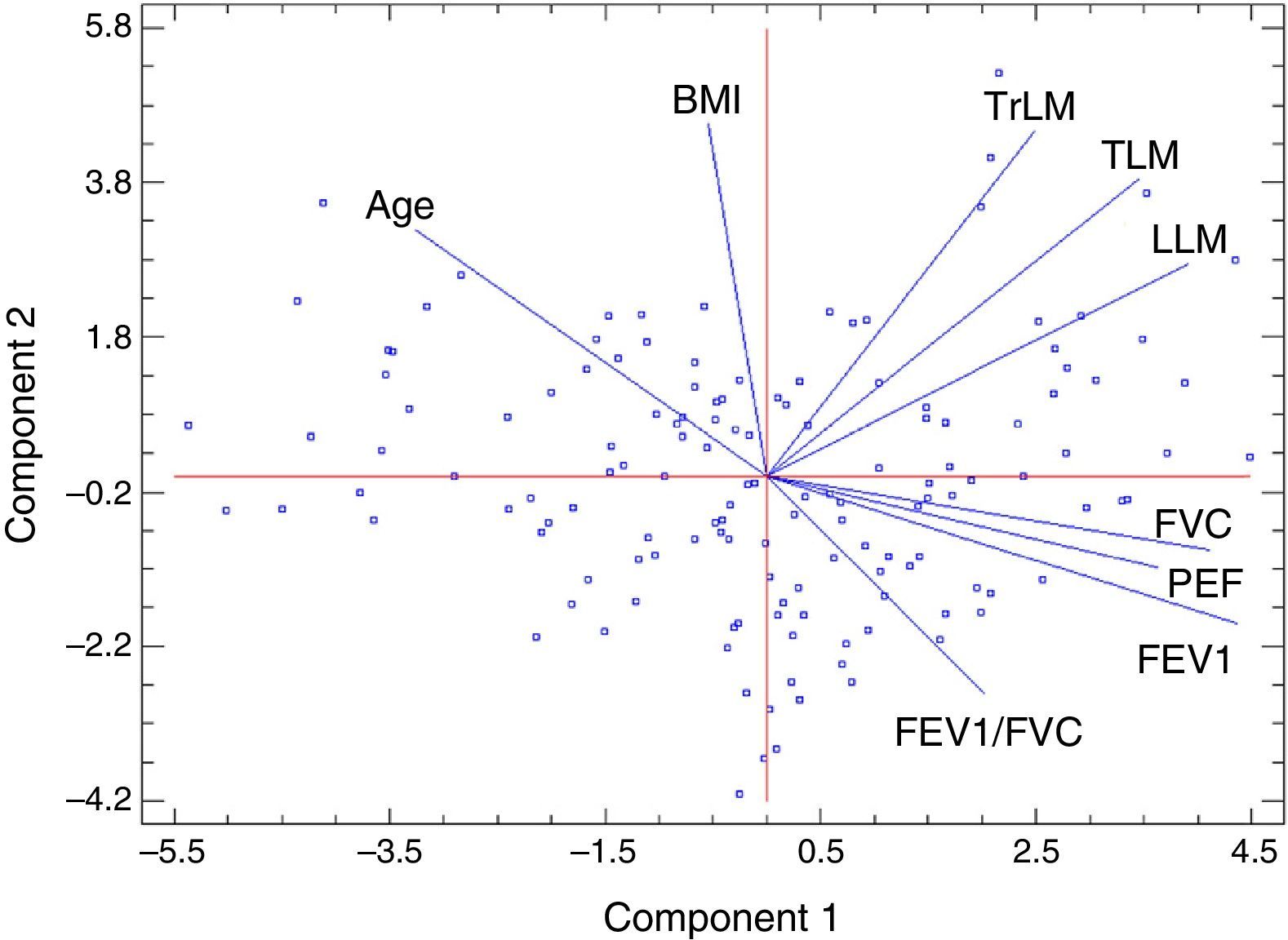
Principal component analysis in men with an overall explanation of 76.07% (47.1% explains the first component and 28.97% the second). FEV1: forced expiratory volume in 1s; FVC: forced vital capacity; BMI: body mass index; PEF: peak expiratory flow; LLM: leg lean mass; TLM: total lean body mass; TrLM: trunk lean mass.
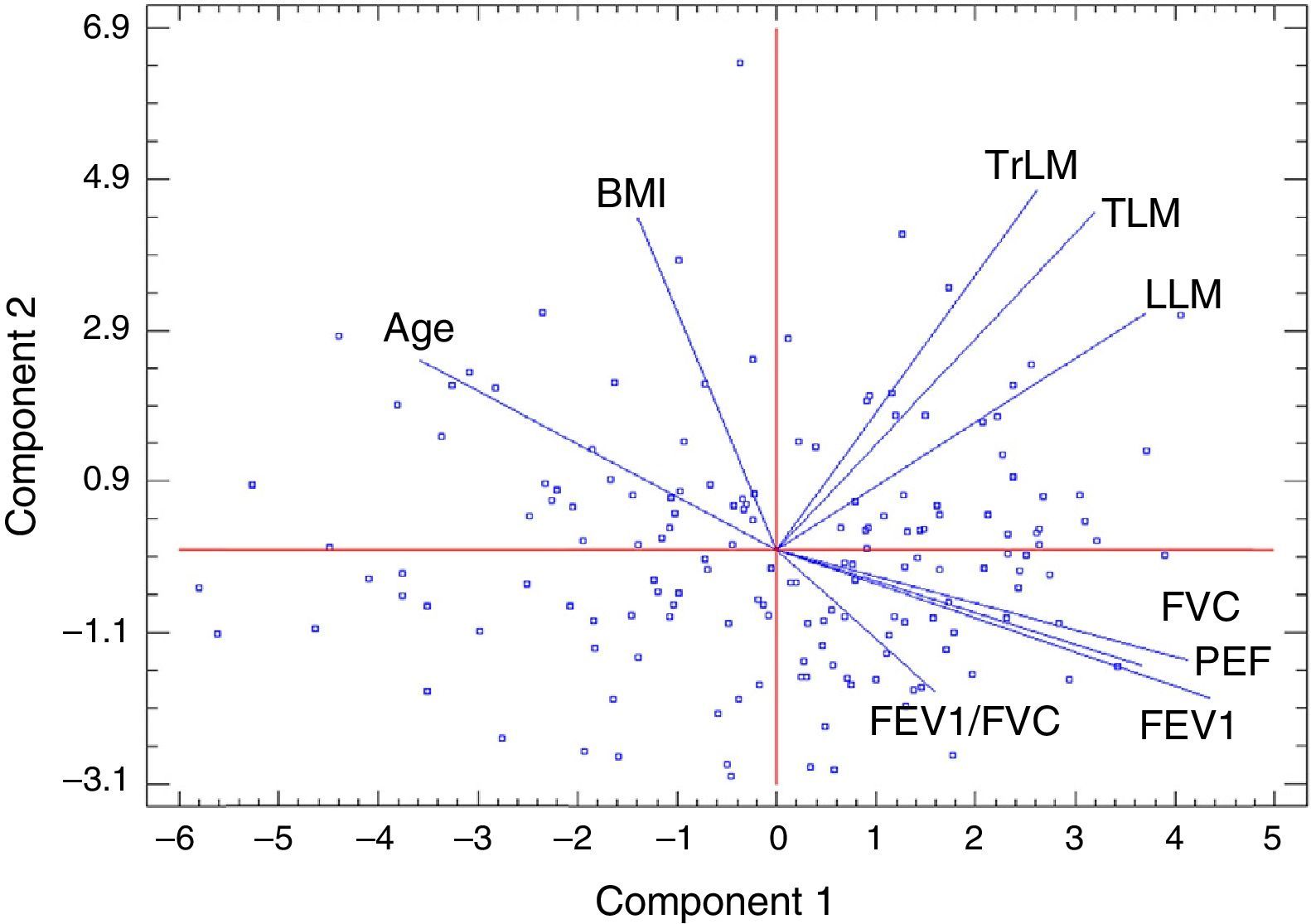
Principal component analysis in women with an overall explanation of 73.03% (46.97% explains the first component and 26.05% the second). FEV1: Forced expiratory volume in 1s; FVC: forced vital capacity; BMI: body mass index; PEF: peak expiratory flow; LLM: leg lean mass; TLM: total lean body mass; TrLM: trunk lean mass.
Partial correlations between lean mass and spirometric variables, adjusting for age and BMI, were positive and highly statistically significant in both women and men, with higher coefficients in the latter (Tables 2 and 3).
Partial Correlation Coefficients Between Muscle Mass Variables and Spirometric Variables Adjusting for Age and Body Mass Index in Men.
| FVC | FEV1 | PEF | FEF25%–75% | FEV1/FVC | |
|---|---|---|---|---|---|
| TLM | 0.603** | 0.583** | 0.371** | 0.310** | −0.098 |
| TrLM | 0.529** | 0.477** | 0.336** | 0.219** | −0.166 |
| LLM | 0.607** | 0.599** | 0.351** | 0.354** | −0.052 |
FEF25%–75%: midexpiratory flow; FEV1: forced expiratory volume in 1s; FVC: forced vital capacity; PEF: peak expiratory flow; LLM: leg lean mass; TLM: total lean body mass; TrLM: trunk lean mass.
Partial Correlation Coefficients Between Muscle Mass Variables and Spirometric Variables Adjusting for Age and Body Mass Index in Women.
| FVC | FEV1 | PEF | FEF25%–75% | FEV1/FVC | |
|---|---|---|---|---|---|
| TLM | 0.367** | 0.341** | 0.206** | 0.165* | −0.103 |
| TrLM (kg) | 0.394** | 0.373** | 0.272** | 0.183* | −0.095 |
| LLM (kg) | 0.359** | 0.337** | 0.178** | 0.167* | −0.094 |
FEF25%–75%: midexpiratory flow; FEV1: forced expiratory volume in 1s; FVC: forced vital capacity; PEF: peak expiratory flow; LLM: leg lean mass; TLM: total lean body mass; TrLM: trunk lean mass.
*p<0.05 is statistically significant.
**p<0.01 is highly statistically significant.
Variables showing higher correlation coefficients with FVC and with FEV1 were LLM in men and TrLM in women.
In the multiple linear regression analysis, equations to predict spirometric variables according to age, BMI and lean mass variables were obtained, along with adjusted coefficients of determination (R2) (Table 4).
Regression Equations and Adjusted R2 Values Obtained in the Multiple Linear Regression Analysis in Men and Women.
| Equation | Sex | Adjusted R2 |
|---|---|---|
| FVC=4159.67−16.4626*Age−66.2774*BMI+0.157654*LLM | M | 61.66 |
| FVC=3496.64−15.6366*Age−37.1272*BMI+0.113454*LLM | F | 47.80 |
| FEV1=3849.83−23.123*Age−50.7761*BMI+0.122798*LLM | M | 71.71 |
| FEV1=3236.55−19.001*Age−26.2374*BMI+0.0844262*LLM | F | 57.96 |
| PEF=7801.62−40.8775*Age−55.4911*BMI+0.234124*LLM | M | 34.29 |
| PEF=6616.24−34.1297*Age−22.0113*BMI+0.127834*LLM | F | 27.87 |
| FVC=4939.19−28.6842*Age−55.5342*BMI+0.0996814*TRLM | M | 56.24 |
| FVC=3672.79−20.372*Age−41.0691*BMI+0.101592*TRLM | F | 49.39 |
| FEV1=4543.92−32.8348*Age−39.124*BMI+0.0710143*TRLM | M | 65.9 |
| FEV1=3362.43−22.5101*Age−29.2664*BMI+0.0760471*TRLM | F | 59.16 |
| PEF=8767.04−58.602*Age−46.8003*BMI+0.162691*TRLM | M | 33.5 |
| PEF=6296.34−37.9955*Age−36.0042*BMI+0.159189*TRLM | F | 31.02 |
| FVC=4211.3−20.8774*Age−74.7347*BMI+0.061934*TLM | M | 61.37 |
| FVC=3470.12−17.8657*Age−42.4918*BMI+0.0487907*TLM | F | 48.16 |
| FEV1=3921.89−26.729*Age−56.2906*BMI+0.047272*TLM | M | 70.8 |
| FEV1=3230.27−20.7168*Age−30.0039*BMI+0.0358316*TLM | F | 58.07 |
| PEF=7686.54−46.4255*Age−74.5144*BMI+0.0978115*TLM | M | 33.36 |
| PEF=6383.31−35.7814*Age−31.457*BMI+0.0621525*TLM | F | 28.67 |
FEV1: forced expiratory volume in 1s; FVC: forced vital capacity; BMI: body mass index; PEF: peak expiratory flow; LLM: leg lean mass; TLM: total lean mass; TrLM: trunk lean mass.
R2 between lean mass and spirometric variables are greater in men. The spirometric variable with the highest values was FEV1, followed by FVC and PEF, in both men and women. In men, LLM is the variable that showed the highest R2 with spirometric variables, while in women, it was TrLM.
All estimated regression coefficients in lean mass were positive and statistically significant (p<0.05), suggesting that the greater the amount of lean body mass, the greater the absolute values obtained on spirometry. The highest coefficients were for LLM in men and TrLM in women.
Discussion and ConclusionsThe aim of this study was to establish the association between spirometric results and lean mass determined by DEXA in healthy individuals. Variability in the spirometry values obtained in healthy individuals of similar characteristics have led some authors1,2 to believe that factors other than sex, age, height, and weight might determine results. Determinants such as inherited genetic factors and the presence of certain vitamins in an individual's diet have been discussed. The premise of this study is that one of the factors that might cause this variability could be muscle mass. Other studies have attempted to establish the influence of the muscle component of the body on spirometric results in healthy individuals:
Cotes et al.3 found a significant association between the Fat-Free Mass Index (FFMI), in which lean mass is adjusted for subject height obtained from anthropometric measurements, and the main spirometric parameters. They used linear regression models to obtain reference equations that included FFMI, and found that these equations were more accurate than those which included only sex, age, height, and weight.
Mohamed et al.4 also measured a muscle mass parameter, bone-free lean body mass (BF-LBM), using DEXA, and, like us, found a significant positive association between that parameter and the main spirometric variables in a group of healthy Italian subjects. The age range is similar, but the series size is rather smaller than ours (58 men and 60 women), and the influence of regional lean mass variables was not studied.
More recently, Lim et al.,5 in a study of elderly Korean individuals with no chronic respiratory diseases, found a significant association between trunk and leg muscle measured by DEXA and the main spirometric parameters, in both women and men. Their results are similar to our findings, although only elderly subjects of non-Caucasian origin were included.
Park et al.6 also conducted a study in Korean subjects, but with a mean age of 46 years. They found a significant correlation between lean body mass – measured in this case by bioelectric impedance – and spirometric parameters, in both men and women. However, they did not obtain a sufficiently high R2 to conclude that muscle mass was a factor that influenced breathing in the study individuals.
Mean values of all respiratory parameters are significantly higher among men than women. The larger amount of total lean body mass in men might explain the difference in the spirometric results between both sexes, taking into account that respiratory mechanical properties are basically the same in both.20 Mean amounts of lean body mass in the different body regions are also higher in men. These results are in line with those of Aguado et al.,21 who determined total and regional lean mass by DEXA in a series of healthy individuals of both sexes, grouped according to age. These authors found consistently larger amounts of total and regional lean body mass in men.
One of the principal results of the study is the significant association of lean mass in the legs with the main spirometric parameters. In men, leg lean mass affected spirometric results even more than total lean mass or trunk lean mass, where the major ventilatory muscles are located. In the clinical setting, Hillman et al.22 believe that muscle strength and muscle mass in the legs are a possible determinant of the efficacy of training programs for pulmonary rehabilitation. They also observed that approximately 33% of patients with COPD presented muscle dysfunction in the lower limbs, even in the early stages of the disease.
While leg lean mass in women is also significantly associated with spirometric parameters, this is not the variable that shows the greatest association. Rather, the amount of muscle mass in the trunk has most impact on spirometric results. This difference between the sexes does not appear to be explained by differences in the regional distribution of lean mass, since no significant differences in this distribution were revealed in the study. In both sexes, the amount of lean mass is greater in the trunk than in the legs, and in similar proportions. The explanation for this difference might be the predominantly thoracic breathing pattern in women.
The possible direct relationship between muscle mass and strength may explain the association between lean mass parameters and spirometric values. This hypothesis is also supported by the fact that a significant association is also found between PEF values, the spirometric parameter most dependent on expiratory muscle strength, and lean mass values, in both men and women. In women, PEF is most associated with trunk mean mass. However, some authors23,24 found that strength does not depend exclusively on muscle mass, and the relationship between these parameters is not linear. The most widely used functional tests for measuring respiratory muscle strength are maximum inspiratory pressure (MIP) and maximum expiratory pressure (MEP). A further study, evaluating the association between lean mass determined by DEXA and MIP and MEP values would help clarify this issue. In this respect, Costes et al.25 found in a study of elderly individuals of both sexes that trunk lean mass determined by DEXA predicts MIP values, but only in women. Hillman et al.22 also found an association between lean mass in the legs and muscle strength determined by dynamometry in COPD patients.
Another result from our study is that all lean mass variables have more effect on FEV1 than on the other spirometric parameters, in both men and women. The greater capacity of the expiratory muscles to generate strength may lead to a greater volume of air being expired in the first second of the forced spirometry maneuver. A positive association is also seen between the amount of lean mass and FEF25%–75%, altered values of which suggest small airway obstruction, and may point to the presence of early-stage obstructive disease. This might mean that a lower mean muscle mass might be a factor in the appearance of obstructive spirometric patterns. In this respect, Minas et al.13 compared muscle mass measured by bioelectric impedance in smokers without COPD and in patients with COPD, and found it to be significantly lower in the latter, even in patients in mild stages of the disease. The same authors studied a group of patients with asthma, another of the most prevalent obstructive diseases. They found that patients with severe treatment-resistant asthma had lower muscle mass measured by bioelectric impedance than those with milder forms of asthma, suggesting that muscle mass may be used as a prognostic factor in these patients.
Another publication reports that up to one third of COPD patients had deteriorated muscle function in the lower limbs, even in the early stages of the disease.26 However, in our study, we did not find a significant association between lean mass parameters and FEV1/FVC index in either sex. We did not find, then, that lower lean mass was a factor for a lower FEV1/FVC index, which would belie the idea that lower muscle mass might be associated with a greater tendency to develop obstructive spirometric patterns.
Spirometric values in healthy individuals are known to peak in the third decade of life, in both men and women. These values then gradually decline with age.27 The course of muscle mass is similar: after reaching a peak, it too declines progressively over the years.28,29 The association between lean mass and spirometric parameters might suggest that loss of muscle mass is one of the factors that might explain the age-related progressive decline in spirometric parameters, as well as deterioration of the mechanical properties of the ribcage and loss of elasticity and distensibility of the alveoli and the airway.
In conclusion, muscle mass has a significant influence on lung function in health individuals of both sexes, but this influence is greater in men.
The amount of lean mass in the legs is the variable that shows closest association with all spirometric parameters in men, while in women, it is trunk lean mass.
In both sexes, lean mass is mainly associated with FEV1 followed by FEV and PEF. However, it is not significantly related with the FEV1/FVC index.
Conflict of InterestsThe authors state that they have no conflict of interests.
Please cite this article as: Martín Holguera R, Turrión Nieves AI, Rodríguez Torres R, Alonso MC. Asociación de la masa muscular determinada mediante DEXA con los resultados espirométricos de individuos sanos. Arch Bronconeumol. 2017;53:375–380.







