



We present a case of acute lung toxicity with eosinophilia due to testosterone cypionate, which to our knowledge is the first case described in the literature.
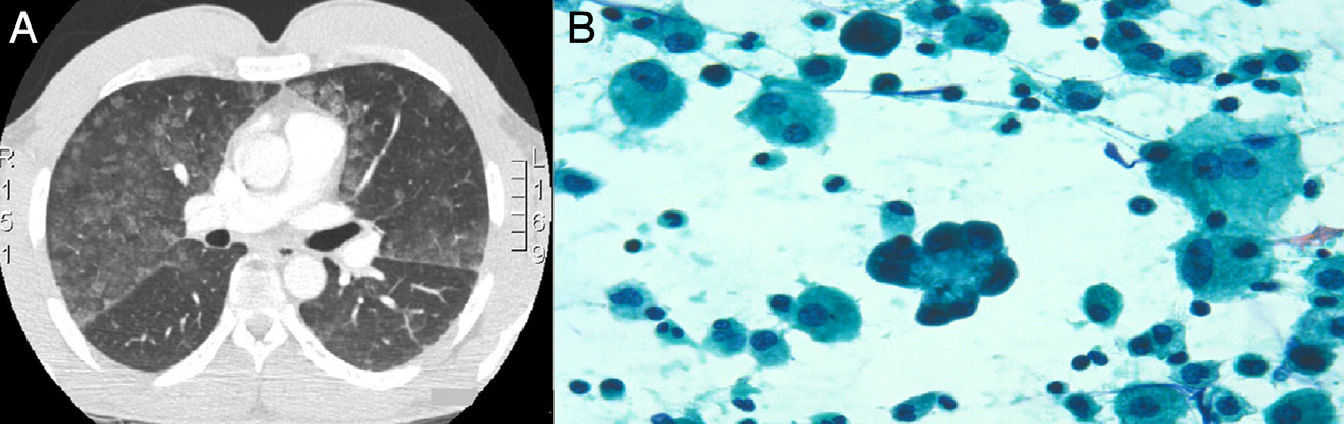
The patient was a 39-year-old male who presented with sudden onset dyspnoea, coughing with a little blood-stained sputum and feeling feverish. Anamnesis: no substance abuse, firefighter by profession. He was involved in bodybuilding during his spare time and had been using hormone supplements intermittently for 20 years. He had begun a new cycle of testosterone cypionate four weeks earlier, taking a weekly dose of 250mg. On the physical examination, he was found to be in general poor health, with profuse sweating, tachypnoea with respiratory rate 28bpm and temperature of 28°C. Auscultation revealed fine crackles in both lung bases. Arterial blood gases: pH 7.44, PaCO2 34mmHg, PaO2 62mmHg. Laboratory tests: complete blood count, leukocytes 19,900μl with predominantly neutrophils (88%, 17600/μl), lymphocytes (4%, 810/μl), eosinophils (0.2%, 40/μl), C-reactive protein 13.3mg/l. Quick index 99%. d-dimer 575ng/ml. Blood glucose, renal function and electrolytes are normal. Serum complement and immunoglobulins are normal. Auto-antibodies test is negative. Chest computed tomography (CT) scan: presence of areas of ground-glass opacity predominantly in bases and dependent regions, septal thickening (Fig. 1a). Fibrobronchoscopy: normal. Microbiological study of the bronchoalveolar lavage (BAL) and bronchial aspirate was negative. Pathological study of the BAL showed a smear with a haematic background and abundant cellularity consisting of alveolar macrophages, with a considerable number of atypical hyperplastic pneumocytes and abundant eosinophils (25%), compatible with a diagnosis of eosinophilia with atypical pneumocyte hyperplasia (Fig. 1b).
Initial treatment was prescribed with oxygen therapy, intravenous levofloxacin and anti-pyretics. On the second day of admission, the patient had symptomatic improvement with disappearance of the dyspnoea and control of the fever; the chest radiograph and arterial blood gases were normal on the fifth day. Two weeks later the patient was asymptomatic and had stopped using hormone supplements. The respiratory function examination, including a diffusion test and chest CT, was normal.
In the clinical setting, androgens are mainly used in testosterone replacement therapy in male hypogonadism.1 The use of testosterone cypionate, despite being banned in competition, is well known in sport for achieving greater strength and enhanced performance, and in bodybuilding for obtaining a rapid increase in muscle mass. In a literature search performed on Pneumotox2 and MEDLINE up to February 2012, we did not find any association between the use of testosterone cypionate and lung toxicity. However, Ramos Villalobos et al.4 reported a case similar to ours caused by the use of methenolone, another anabolic substance used in bodybuilding.
The causal relationship with the drug, presence of infiltrates and confirmation of tissue eosinophilia by BAL led us to consider the possibility of lung toxicity,3 having ruled out other infectious, vascular, autoimmune and immunological conditions. In fact, in our case, there was a temporal relationship to the start of four weeks testosterone cypionate therapy from the first dose, and the symptomatology coincided with the recent use of the following dose, which corresponded to the patient according to the cycle that he had been following. Furthermore, he improved rapidly when the drug was withdrawn, with radiology and respiratory function returning to normal. It is important to highlight that systemic corticosteroids were not used.
As often happens with drug-induced lung toxicity, the patient was admitted with suspected community-acquired pneumonia, although this diagnosis was not confirmed either by microbiological studies or the subsequent evolution. In drug-induced lung disease, high resolution CT shows histological findings that resemble those in other entities such as infection and pulmonary fibrosis.5 The finding of eosinophilia in the BAL reinforced the hypothesis of drug toxicity.6
In conclusion, the current case together with the case reported recently by Ramos Villalobos et al.4 could provide evidence to indicate that the use of testosterone-derived anabolic substances for sport can cause lung toxicity. Attention should be paid in the future to the use of these substances and their possible relationship with physiopathological changes that lead to lesions in the lung parenchyma.
Conflict of InterestsThe authors declare that they have no conflict of interests.
Please cite this article as: Monclou Garzón E, Carrión Valero F, Urbano Salcedo A. Eosinofilia pulmonar por cipionato de testosterona. Arch Bronconeumol. 2013;49:498–499.







