



We present the case of a 77-year-old patient with a history of hypertension and glaucoma, who was admitted to our hospital for symptoms of dyspnea at rest, with no cough or expectoration. As a casual finding on the chest radiograph (Fig. 1A and B), a saccular image was observed with well-defined borders at the level of the left hilum (arrows 1A), extending toward the retrosternal space (arrow 1B). It was decided to complete the study with chest-computed tomography (CT) with intravenous iodated contrast (Fig. 1C and D), in which an aneurysmatic dilatation of the conus arteriosus, 75mm in diameter (p), was reported, with no other findings of interest. Due to the patient's clinical history (asymptomatic, located in the pulmonary trunk, with no data indicating a high risk of rupture), it was decided to opt for a conservative approach to the aneurysm.
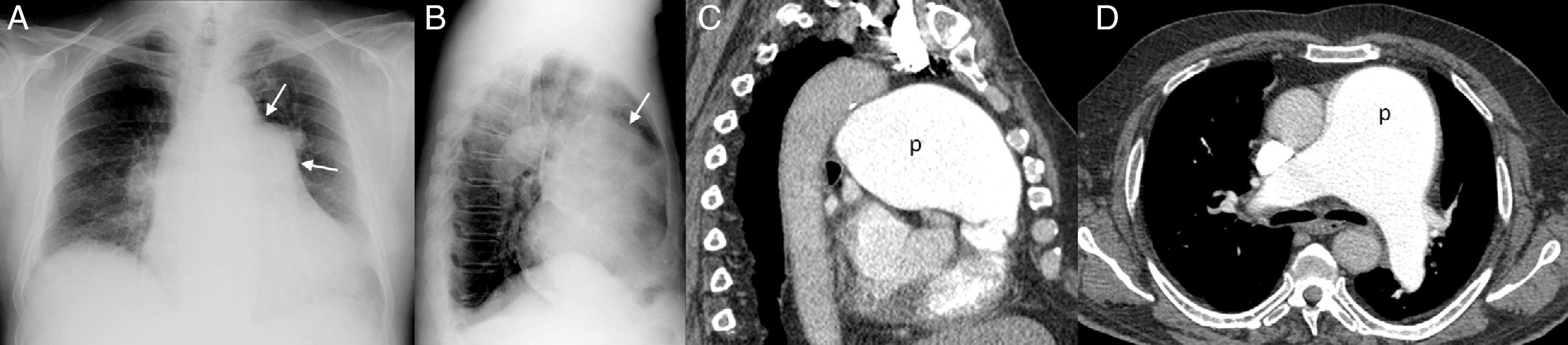
Chest X-ray, posterior–anterior (PA) (A) and lateral (B), in which a smooth rounded lesion at the level of the left hilum can be seen in the PA projection (arrows 1A), projecting into the retrosternal space (arrow 1B). Chest CT with the administration of intravenous contrast, sagittal and axial projection (C and D) confirms an aneurysmatic dilatation of the conus arteriosus.
Pulmonary artery aneurysms are rare entities1 and are difficult to diagnose due to their low prevalence, as they often present with non-specific symptoms or even in asymptomatic patients.2 Only isolated cases have been documented in the world literature, and their management remains unclear.
Please cite this article as: Mayoral-Campos V, de Benito-Arévalo JL, Varea-Sanz MA. Aneurisma de la arteria pulmonar. Arch Bronconeumol. 2013;49:551–552.







