



Intercostal hernia is a very rare disorder which is mainly described in the context of trauma or following thoracic surgery.1,2 Depending on their aetiology, intercostal hernias can be classified as acquired (traumatic, spontaneous or pathological) or congenital.2 Post-operative thoracic hernias are usually a result of inadequate closure of the chest wall.2 However, most patients present hernia of the lung,1,2 defined as a protrusion of lung tissue beyond the confines of the chest cavity.3 In contrast, the protrusion of soft tissue into the pleural cavity (inverted intercostal hernia) is extremely rare.1 Here we describe a case of this type, highlighting the findings observed on multidetector computed tomography (MDCT).
A 45-year-old woman was admitted with a 10-day history of chest pain in the posterior part of the right side, with no other associated symptoms. Ten years earlier, she had undergone resection of the seventh rib due to a costal hemangioma. A MDCT was performed, which revealed the presence of a convex lens-shaped herniation and incarceration of soft tissue of the right posterior chest wall (subcutaneous fat layer and major rhomboid muscle) in the pleural cavity through a widened intercostal space between the sixth and eighth ribs (Fig. 1). The thoracic surgeon responsible for the treatment opted to perform an exploratory thoracotomy via this interspace, but no masses were observed in the chest wall during the procedure. The thoracotomy incision was closed carefully with strong stitches to prevent recurrence of the hernia. Post-operative recovery was uneventful and the patient was discharged with no symptoms.
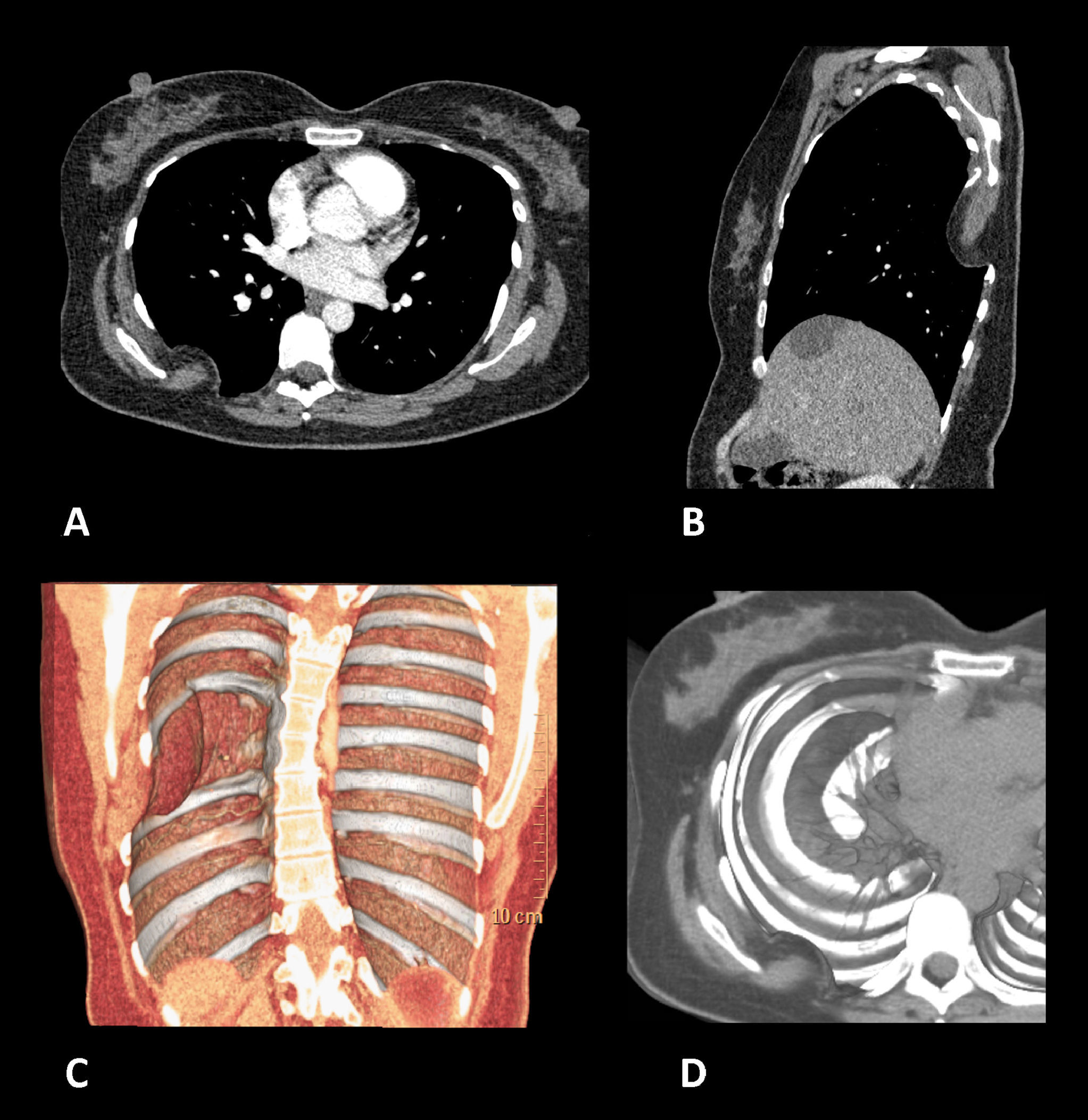
Axial (A) and sagittal (B) CT with contrast, with reconstructions (C,D), in which a convex lens-shaped herniation and incarceration of soft tissue of the right posterior wall of the thorax (subcutaneous fat layer and major rhomboid muscle) can be observed in the pleural cavity via the widened space between the sixth and eighth ribs.
Inverted intercostal hernia of soft tissue of the chest wall is an extremely rare disorder.1 Although it would be expected that the negative pressure in the pleural cavity could lead to a protrusion of the soft tissue of the chest wall into the pleural cavity via an intercostal space that has been widened in patients who have undergone chest surgery,1 it has been reported that the muscle tension in the chest wall is sufficient to prevent this complication.1 Iwata et al.1 recently described a case of inverted intercostal hernia of soft tissue of the back that simulated a slow-growing chest wall tumour in an 80-year-old woman who had undergone a thoracotomy to treat a benign lesion 11 years previously. In this case, the authors attributed the appearance of the herniation to progressive muscle weakness caused by the patient's age.1 In our case, since the clinical manifestations of chest pain and the diagnosis occurred 10 years after the thoracic surgery, progressive muscle weakness is a possibility, although inadequate closure of the chest wall is also a likely hypothesis. However, unlike the case of Iwata et al.,1 which manifested with a predominantly hypodense mass in the chest wall observed on the CT, the CT findings in our case were obvious and clearly showed the components of the hernia (subcutaneous fat and major rhomboid muscle), so the preoperative diagnosis was unequivocal.
FundingNone.
Conflict of InterestsThe authors declare that they have no conflict of interests.
Please cite this article as: Torres US, Portela-Oliveira E, del Campo Braojos F, Vargas Cardoso L, Soares Souza Jr. A. Hernia intercostal invertida de tejido blando de la pared torácica: hallazgos en la tomografía computarizada multidetector. Arch Bronconeumol. 2013;49:553–554.







