

To investigate the burden of asthma in a young adult population in urban areas of Argentina.
DesignA nationwide telephone survey in subjects aged 20–44 years was performed in urban areas in Argentina. The European Community Respiratory Health Survey questionnaire was used. Asthma was defined as an exacerbation in the last year or use of asthma medications.
ResultsIn total, 1521 subjects responded (62.4% females, mean age 33 years), of whom 91 were classified as asthmatics (5.9%, 95% CI 4.7–7.1). Prevalence adjusted for age, sex and education level was 6.4% (95% CI 5.1–7.7). Wheezing was reported by 13.9% (95% CI 15.6–12.2) and a diagnosis of asthma by 9.5% (95% CI 8.0–11.0). Among individuals with a diagnosis of asthma (n=154), 71.3% had undergone spirometry. Among those treated (n=77), 51.9% used medications daily and 46.8% as a rescue measure. Of those reporting an exacerbation in the last year (n=60), 55% had attended an emergency department and 23% were admitted. Asthma was associated with rhinitis (OR 11.1, 95% CI 6.2–19.9) and family history (OR 3.6, 95% CI 2.3–5.5).
ConclusionAsthma prevalence in young adults in Argentina is similar to Europe. Although attacks and admissions were common, regular use of medications was reported by half of those treated. These results may be useful for other Latin American countries.
Estimar la carga del asma en la población adulta joven en zonas urbanas de Argentina.
DiseñoSe realizó una encuesta telefónica a nivel nacional en sujetos de 20 a 44 años en áreas urbanas de Argentina. Se utilizó el cuestionario de la European Community Respiratory Health Survey. El asma se definió como ataque en el último año o uso de medicamentos para el asma.
ResultadosMil quinientos veintiún sujetos fueron encuestados (62,4% mujeres, edad media 33 años). Noventa y uno fueron clasificados como asmáticos (5,9%, IC 95% 4,7-7,1). La prevalencia ajustada por edad, sexo y nivel educativo fue de 6,4% (IC 95% 5,1-7,7). El porcentaje de sibilancia fue de un 13,9% (IC 95% 15,6-12,2) y el de diagnóstico médico de asma, de un 9,5% (IC 95% 8,0-11,0). Entre los diagnósticos (n=154), el 71,3% realizó una espirometría y el 51,9% de los tratados (n=77) utilizaba medicamentos diariamente y un 46,8% como rescate. De los que reportaron algún ataque en el último año (n=60), un 55% tuvieron una visita a Urgencias y un 23,3% fueron hospitalizados. El asma se asoció con rinitis (OR 11,1; IC 95% 6,2-19,9) e historia familiar (OR 3,6; IC 95% 2,3-5,5).
ConclusiónLa prevalencia de asma en adultos jóvenes en Argentina es similar a la de Europa. Aunque los ataques y las admisiones fueron comunes, el uso regular de los medicamentos fue informado por la mitad de los tratados. Los resultados pueden ser útiles para otros países de América Latina.
The World Health Organization has warned that the prevalence of asthma is on the rise in many regions of the world, and that this disease is the most common chronic illness in children.1 It is estimated that asthma affects more than 300 million people around the world, causing approximately 250000 deaths per year.2
Asthma is highly prevalent in many cities in Latin America, as reported by the International Study of Asthma and Allergies in Childhood (ISAAC).3 In Latin America, asthma mortality rates were high in the 1980s, but a gradual decline was subsequently observed in most of the countries studied, probably due to changes in therapeutic management and increased prescription of anti-inflammatory drugs.4–8 Asthma is one of the 10 leading causes of years lived with disability in several countries in Latin America.9
The ISAAC study, conducted in 1995, reported a 15.4% and 17.3% prevalence of wheezing among Argentine children aged 6–7 years living in Buenos Aires and Rosario, respectively.10 In 2001, prevalence among the group aged 13–14 years was 9.9% in Buenos Aires, 11.8% in Rosario, and 11.2% in Cordoba. Phase 3 of the study was performed in Cordoba, where an increase in prevalence of up to 13.6% was reported.4
Prevalence studies in adult asthma are hampered by the definition of the disease, so to determine its prevalence, methodologies proven reliable in other regions must be used.11
Despite the difficulties and the complexity of defining the problem and how to measure it, collecting data on the epidemiological situation of asthma will allow priorities and at-risk populations to be identified and will pave the way for public health.
Given the significant burden of asthma morbidity in Argentina and the need to clarify the situation in young adults, this study was conducted to estimate the prevalence of asthma among individuals aged 20–44 years, and to evaluate the characteristics of care and disease determinants.
Materials and MethodsA cross-sectional study was conducted in a population aged 20–44 years, in 28 cities with at least 100000 inhabitants throughout the Republic of Argentina, between October and December 2014.
A structured questionnaire with 22 closed questions was administered. This was a shortened version of the previously validated Spanish version of the European Community Respiratory Health Survey (ECRHS) questionnaire.12–15 The questionnaire was administered in a telephone call, on landlines, using the computer-assisted telephone interviewing (CATI) system. Subjects who gave their verbal consent were included in the study.
The questionnaire included demographic information (age, sex, province, city, healthcare coverage, occupation, education), asthma symptoms (wheezing, chest tightness, dyspnea, cough), asthma care characteristics (medical attention during asthma attacks, asthma medication), smoking (history of exposure to tobacco smoke, smoking habit), anthropometric characteristics (weight and height), and physical activity (frequency).
The sample size was set at 1500 respondents assuming a prevalence of asthma of 4%, as determined by the ECRHS in a population of the same age range.15 Individuals were selected by simple random sampling, stratified by geographic area.
An individual with asthma was defined as one who responded in the affirmative to any of the following questions: “Have you had an asthma attack in the last 12 months?”, or “Are you currently taking asthma medication?”.14,16,17 The prevalence of wheezing was also based on a positive response to the following question: “Have you had wheezing or whistling in the chest in the last 12 months?”. The presence of asthma according to the ECRHS definition was also determined: having had an asthma attack, use of medications for asthma, or waking in the night with a feeling of chest tightness or oppression any time in the last 12 months.14,17 To correct for the difference in the surveyed population and the general population of the country, asthma prevalence rates adjusted for age, sex, and level of education were calculated for each of the definitions used, along with their 95% confidence intervals. Adjustment was made by the direct method, using the population of Argentina from the census of 2010 as the reference population.
The characteristics of the cases that met the definition of asthma were described by calculating the percentages of the characteristics studied, along with the confidence interval. The association between the presence of asthma according to the definition used and these characteristics was evaluated by calculating the odds ratio and the 95% confidence interval.
The asymptotic approximation to the normal distribution or the exact method were used to calculate confidence intervals of the percentages, and the Woolf method was used for the odds ratio.
Data were loaded into a central database for analysis. MS Excel 2013 and IBM SPSS Statistics 21 were used for the preparation of tables and statistical analysis.
This study was approved by the Ethics and Safety Advisory Research Committee of the Universidad Nacional del Litoral. All participants were asked to give their recorded verbal consent, which was read in the same way for all respondents, and if subjects agreed to participate, they were asked to indicate this clearly in the recording, and to confirm, for the record, that any doubts or additional questions had been resolved before consent was given. The data collected were transferred to a database from which all information relating to the identification of subjects was deleted to ensure their anonymity; all investigators with access to personal data from the respondents were also required to sign a non-disclosure agreement.
ResultsA total of 5283 phone calls were made in the 28 cities; 2252 respondents fell outside the age range for this study, 72 did not give their age, and 2959 were in the appropriate age group. Of these 2959, 1438 did not give their consent to the survey. Distribution of the 1521 individuals interviewed met the proportional distribution per city (Fig. 1).

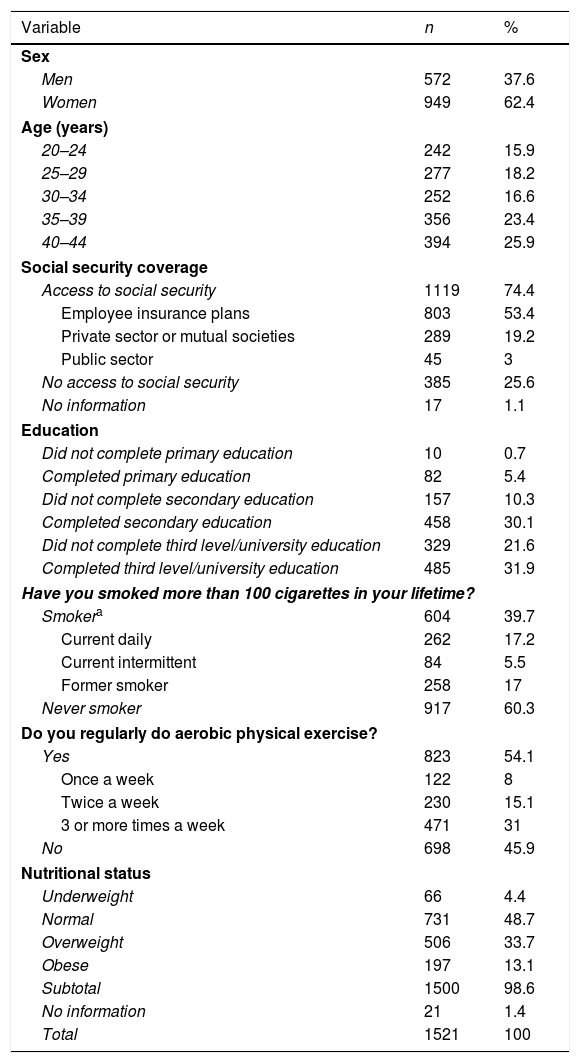
Table 1 shows the distribution of the general characteristics of the population. Women were predominant in all age groups: 55.9% among individuals younger than 35 years, and 69.1% among those 35 years of age or more.
Study Population Demographics and Lifestyle (n=1521).
| Variable | n | % |
|---|---|---|
| Sex | ||
| Men | 572 | 37.6 |
| Women | 949 | 62.4 |
| Age (years) | ||
| 20–24 | 242 | 15.9 |
| 25–29 | 277 | 18.2 |
| 30–34 | 252 | 16.6 |
| 35–39 | 356 | 23.4 |
| 40–44 | 394 | 25.9 |
| Social security coverage | ||
| Access to social security | 1119 | 74.4 |
| Employee insurance plans | 803 | 53.4 |
| Private sector or mutual societies | 289 | 19.2 |
| Public sector | 45 | 3 |
| No access to social security | 385 | 25.6 |
| No information | 17 | 1.1 |
| Education | ||
| Did not complete primary education | 10 | 0.7 |
| Completed primary education | 82 | 5.4 |
| Did not complete secondary education | 157 | 10.3 |
| Completed secondary education | 458 | 30.1 |
| Did not complete third level/university education | 329 | 21.6 |
| Completed third level/university education | 485 | 31.9 |
| Have you smoked more than 100 cigarettes in your lifetime? | ||
| Smokera | 604 | 39.7 |
| Current daily | 262 | 17.2 |
| Current intermittent | 84 | 5.5 |
| Former smoker | 258 | 17 |
| Never smoker | 917 | 60.3 |
| Do you regularly do aerobic physical exercise? | ||
| Yes | 823 | 54.1 |
| Once a week | 122 | 8 |
| Twice a week | 230 | 15.1 |
| 3 or more times a week | 471 | 31 |
| No | 698 | 45.9 |
| Nutritional status | ||
| Underweight | 66 | 4.4 |
| Normal | 731 | 48.7 |
| Overweight | 506 | 33.7 |
| Obese | 197 | 13.1 |
| Subtotal | 1500 | 98.6 |
| No information | 21 | 1.4 |
| Total | 1521 | 100 |
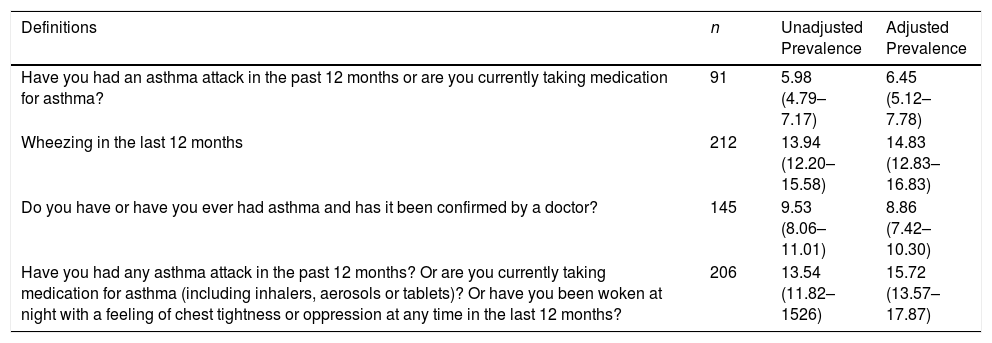
With regard to asthma prevalence, 5.9% (95% CI 4.7–7.1) of the population surveyed answered that they had had an asthma attack in the past 12 months or were currently taking asthma medication. Asthma prevalence adjusted for sex, age, and educational level in Argentina was 6.4% (95% CI 5.1–7.7) (Table 2).
Adjusted and Adjusted Prevalence of Asthma According to Different Definitions.
| Definitions | n | Unadjusted Prevalence | Adjusted Prevalence |
|---|---|---|---|
| Have you had an asthma attack in the past 12 months or are you currently taking medication for asthma? | 91 | 5.98 (4.79–7.17) | 6.45 (5.12–7.78) |
| Wheezing in the last 12 months | 212 | 13.94 (12.20–15.58) | 14.83 (12.83–16.83) |
| Do you have or have you ever had asthma and has it been confirmed by a doctor? | 145 | 9.53 (8.06–11.01) | 8.86 (7.42–10.30) |
| Have you had any asthma attack in the past 12 months? Or are you currently taking medication for asthma (including inhalers, aerosols or tablets)? Or have you been woken at night with a feeling of chest tightness or oppression at any time in the last 12 months? | 206 | 13.54 (11.82–1526) | 15.72 (13.57–17.87) |
Source: National survey of the prevalence of asthma in adults. Argentina, 2015.
The proportion of individuals who reported an episode of wheezing in the last 12 months was more than double the prevalence observed for asthma (13.9%; 95% CI 12.2–15.6), and the proportion of individuals diagnosed by doctors was 60% higher (9.5%; 95% CI 8.0–11.0).
Finally, if asthma prevalence is calculated using the ECRHS definition (that includes being woken in the night with a sensation of chest tightness in the past 12 months) instead of the study definition, rates (both adjusted and unadjusted) more than double (15.72; 95% CI 13.3–17.8, and 13.5; 95% CI 11.8–15.2). Adjusted rates were all higher than the unadjusted rates, except for the definition corresponding to asthma diagnosed by a doctor, which was lower.
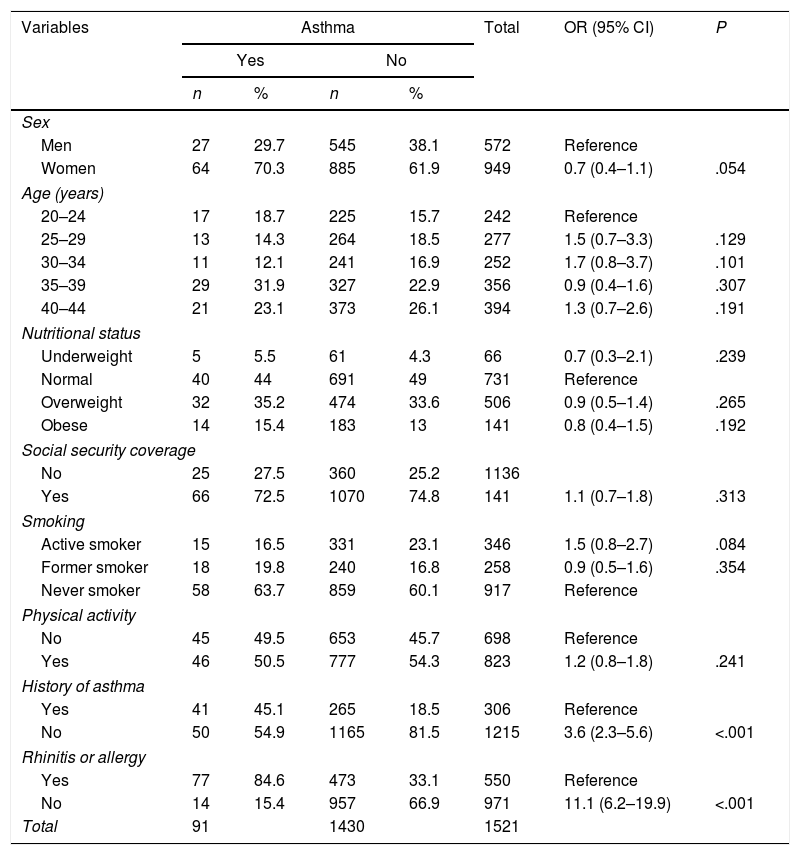
The characteristics of individuals classified as asthmatic and non-asthmatic are shown in Table 3. The distribution of general and personal characteristics was similar in the respondents classified as asthmatics and non-asthmatics, and no statistically significant differences were observed between groups in terms of sex, age, nutritional status, social security coverage, smoking habit, and physical activity. In contrast, the association between asthma and reported history (family history of asthma and allergic rhinitis) was high and statistically significant.
Comparison of Subjects According to the Absence or Presence of Asthma (n=1521).
| Variables | Asthma | Total | OR (95% CI) | P | |||
|---|---|---|---|---|---|---|---|
| Yes | No | ||||||
| n | % | n | % | ||||
| Sex | |||||||
| Men | 27 | 29.7 | 545 | 38.1 | 572 | Reference | |
| Women | 64 | 70.3 | 885 | 61.9 | 949 | 0.7 (0.4–1.1) | .054 |
| Age (years) | |||||||
| 20–24 | 17 | 18.7 | 225 | 15.7 | 242 | Reference | |
| 25–29 | 13 | 14.3 | 264 | 18.5 | 277 | 1.5 (0.7–3.3) | .129 |
| 30–34 | 11 | 12.1 | 241 | 16.9 | 252 | 1.7 (0.8–3.7) | .101 |
| 35–39 | 29 | 31.9 | 327 | 22.9 | 356 | 0.9 (0.4–1.6) | .307 |
| 40–44 | 21 | 23.1 | 373 | 26.1 | 394 | 1.3 (0.7–2.6) | .191 |
| Nutritional status | |||||||
| Underweight | 5 | 5.5 | 61 | 4.3 | 66 | 0.7 (0.3–2.1) | .239 |
| Normal | 40 | 44 | 691 | 49 | 731 | Reference | |
| Overweight | 32 | 35.2 | 474 | 33.6 | 506 | 0.9 (0.5–1.4) | .265 |
| Obese | 14 | 15.4 | 183 | 13 | 141 | 0.8 (0.4–1.5) | .192 |
| Social security coverage | |||||||
| No | 25 | 27.5 | 360 | 25.2 | 1136 | ||
| Yes | 66 | 72.5 | 1070 | 74.8 | 141 | 1.1 (0.7–1.8) | .313 |
| Smoking | |||||||
| Active smoker | 15 | 16.5 | 331 | 23.1 | 346 | 1.5 (0.8–2.7) | .084 |
| Former smoker | 18 | 19.8 | 240 | 16.8 | 258 | 0.9 (0.5–1.6) | .354 |
| Never smoker | 58 | 63.7 | 859 | 60.1 | 917 | Reference | |
| Physical activity | |||||||
| No | 45 | 49.5 | 653 | 45.7 | 698 | Reference | |
| Yes | 46 | 50.5 | 777 | 54.3 | 823 | 1.2 (0.8–1.8) | .241 |
| History of asthma | |||||||
| Yes | 41 | 45.1 | 265 | 18.5 | 306 | Reference | |
| No | 50 | 54.9 | 1165 | 81.5 | 1215 | 3.6 (2.3–5.6) | <.001 |
| Rhinitis or allergy | |||||||
| Yes | 77 | 84.6 | 473 | 33.1 | 550 | Reference | |
| No | 14 | 15.4 | 957 | 66.9 | 971 | 11.1 (6.2–19.9) | <.001 |
| Total | 91 | 1430 | 1521 | ||||
Source: National survey of the prevalence of asthma in adults. Argentina, 2015.
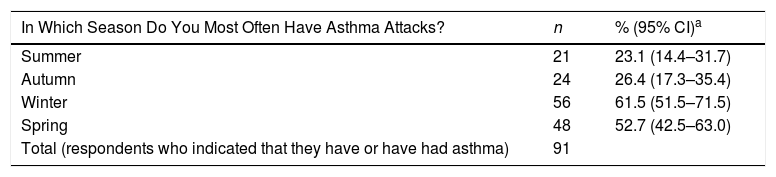
When the frequency of asthma exacerbations was analyzed by season of the year, exacerbations were found to be more predominant in winter and spring than in summer or autumn (Table 4).
Frequency of Asthma Attacks Per Season (n=91 Asthma Patients).
| In Which Season Do You Most Often Have Asthma Attacks? | n | % (95% CI)a |
|---|---|---|
| Summer | 21 | 23.1 (14.4–31.7) |
| Autumn | 24 | 26.4 (17.3–35.4) |
| Winter | 56 | 61.5 (51.5–71.5) |
| Spring | 48 | 52.7 (42.5–63.0) |
| Total (respondents who indicated that they have or have had asthma) | 91 |
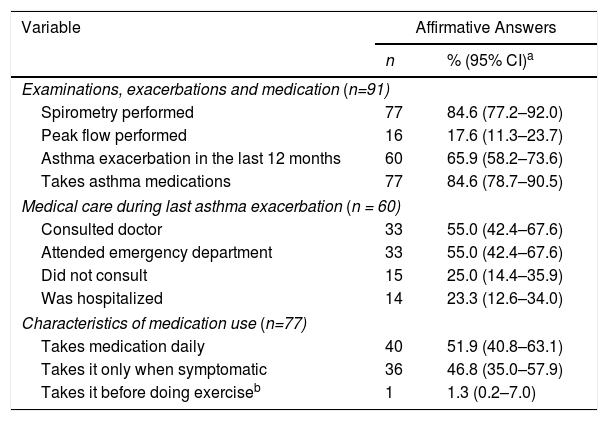
Finally, Table 5 shows data on the diagnosis, medical care and management of the asthma exacerbation, and the treatment modality.
Medical Care, Management of Exacerbations and Use of Therapy in Asthma.
| Variable | Affirmative Answers | |
|---|---|---|
| n | % (95% CI)a | |
| Examinations, exacerbations and medication (n=91) | ||
| Spirometry performed | 77 | 84.6 (77.2–92.0) |
| Peak flow performed | 16 | 17.6 (11.3–23.7) |
| Asthma exacerbation in the last 12 months | 60 | 65.9 (58.2–73.6) |
| Takes asthma medications | 77 | 84.6 (78.7–90.5) |
| Medical care during last asthma exacerbation (n = 60) | ||
| Consulted doctor | 33 | 55.0 (42.4–67.6) |
| Attended emergency department | 33 | 55.0 (42.4–67.6) |
| Did not consult | 15 | 25.0 (14.4–35.9) |
| Was hospitalized | 14 | 23.3 (12.6–34.0) |
| Characteristics of medication use (n=77) | ||
| Takes medication daily | 40 | 51.9 (40.8–63.1) |
| Takes it only when symptomatic | 36 | 46.8 (35.0–57.9) |
| Takes it before doing exerciseb | 1 | 1.3 (0.2–7.0) |
As can be seen in Table 5, individuals who meet the definition of asthma have often undergone spirometry testing and usually take asthma medication.
The same percentage of individuals (55% of respondents) consulted their doctor or attended an emergency department for the management of their last asthma exacerbation. Of these, 21 (35%) both consulted their doctor and visited the emergency department. However, 25% did not seek medical attention. In total, 23.3% of the respondents with exacerbations in the last 12 months were hospitalized.
DiscussionThe prevalence of asthma in adults in Latin America has rarely been investigated in the literature, and this situation must be remedied.18,19
This is probably due to several factors, such as the lack of a globally accepted definition of asthma in epidemiological studies and differences in the perception of asthma symptoms across different socioeconomic strata.18
In this study, we used the Global Atlas of Asthma18 definition to compare the prevalence of asthma in Argentina with other regions around the world.
In Argentina, adjusted asthma prevalence was 6.4% in the group aged 20–44 years. This value was similar to that of cities in France, Spain, and Portugal, and lower than cities in New Zealand and Australia. The figures could not be compared with other Latin American cities, because no studies have been performed using the same definition of asthma.18
In Mexico, the prevalence of asthma among individuals over 40 years of age was 5%, but this estimate was determined from the Platino study questionnaire, an instrument designed to evaluate the prevalence of COPD.19
The adjusted prevalence of wheezing was 14.8%. Reliable data on the prevalence of wheezing in the adult population are as scant and unclear as the definition of asthma. In Colombia, in 2009–2010, a study using the ISAAC questionnaire and the same definition of asthma in the 18–59-year age group found a 9.7% prevalence of wheezing.17
Prevalence of asthma diagnosed by doctors was 9.3%, approximately one third lower than in the United States,17 and as mentioned in the results section, about two thirds higher than the prevalence of asthma based on the definition used in our study. It is very likely that some of these patients had been diagnosed with asthma in childhood or adolescence, but were disease-free at the time of the survey.
Figures on smoking and excess weight are similar to those obtained in the latest National Survey of Risk Factors (ENFR 2013), in which 37.4% of patients had a history of smoking, and 25.1%20 were current smokers, compared to 39.7% and 17.2% in this study, respectively. The ENFR 2013 found that 37.1% of patients were overweight, compared to 33.7% in this study, and when obesity was analyzed, more of our patients were obese: 20.8% in our study compared to 13.1% in the ENFR.
Tobacco exposure, both in smokers and those exposed to second-hand smoke, has been associated with asthma by several authors, but we did not observe this association in our study. This could be because our sample size was too small to detect differences between groups according to their tobacco use, or because of the lack of correlation observed in cross-sectional studies between tobacco use and asthma prevalence. The same situation was found with regard to the nutritional status of the respondents, since other studies have shown a link between excess weight and obesity and asthma that was not detected in this study.21,22
The percentage of individuals in our study who did not engage in regular physical activity was similar to that of the ENFR, in which 46.3% of respondents aged 18–24 years and 49% of those aged 25–39 years did not perform regular exercise. The figures obtained in our survey were similar: 45.9% for the overall sample.
A total of 50.6% of patients who met the definition for asthma engaged in physical activity. This percentage is low, given that the Global Initiative for Asthma (GINA) guidelines recommend aerobic physical activity for asthma patients.23
The close association with allergic rhinitis underlines the importance of diagnosing and concomitantly treating this upper airway disease, as recommended by the ARIA guidelines.24,25
With regard to the management of asthma, it is important to point out that 71.3% of patients with diagnosed asthma had undergone spirometry. This figure is higher than that of other Latin American countries, in line with reports from the Asthma Insights and Reality in Latin America (AIRLA)26 and Asthma Insight and Management (AIM)27 studies. This could be associated with the introduction in 1995 of the GINA Global Strategy for Asthma Management and Prevention document in Argentina, aimed at improving the diagnosis and treatment of asthma by primary care physicians, clinicians and pediatricians.9,28 The introduction of these guidelines may also be related with the increased prescription of inhaled corticosteroids, alone or in combination with long-acting bronchodilators, as occurred in Spain in the 1990s.29
In total, 84% of patients reported taking medication for their asthma, but only 51.9% did so on a daily basis and 46.8% only took medication when they had symptoms. This may be associated with the fact that 65.9% had asthma exacerbations; these occurred more often in winter and spring, and 23% of patients were hospitalized during their last exacerbations.
The high percentage of hospitalization among patients with exacerbations is in line with previous reports from the AIRLA28 and AIM29 studies. A key issue to improve asthma control is to increase treatment adherence, because studies previously performed in Latin America show a compliance rate of only 50% in moderate to severe asthma,30 a figure similar to that observed worldwide.31,32
The distribution of the respondent population was compared to the overall population of the country, given the selected telephone survey methodology. This method was used in previous studies,28,32,33 but runs the risk of selecting a population sample that does not reflect the general population. Nevertheless, our interviewed population can be considered to be widely representative, given that landlines are widespread in Argentina, namely, in 68.2% of the selected cities,33 and that the cities included account for approximately 70% of the country's population.34 Despite the representativeness of the sample, the age and sex distribution differs from that of the general population, and these differences are statistically significant. Representativeness may also be affected by differences in the distribution of socioeconomic levels of our sample compared to the general population. This may be due to the lower proportion of landlines in the homes of individuals with lower social status. Some attempt was made to correct these differences between the sample and the general population using the rate adjustment procedure. With this adjustment, the prevalence of asthma was almost 8% higher than the unadjusted prevalence, which might indicate that the survey slightly underestimates the prevalence of asthma in the population.
Another limitation of our study is that the rural population, which has different causative factors and determinants from urban areas, was not included in the survey. However, there is no overall agreement regarding differences in prevalence in rural and urban areas.
Although no test was performed to confirm the diagnosis of asthma, the ECHRS previously showed an acceptable external validity for the instruments used,14,17 and our results are in line with earlier studies carried out in the field.20,21
ConclusionsAsthma is a prevalent disease among young adults in Argentina. The prevalence of the disease is comparable to that of other countries, but the burden of care for exacerbations is greater and the use of preventive therapy remains low. These findings highlight the need for steps to improve access to medication and patient education. They also highlight the need for training among medical staff, especially in primary care, to improve the delivery of care. We have also demonstrated the importance of performing a study on the burden and characteristics of asthma in a population of young adults, a group that is not generally given priority, to the extent that we were unable to find similar published studies in other Latin American countries. Studies with normalization procedures and weighting provide information on the magnitude of the problem in Argentina and inspire other groups to undertake similar studies in other countries that would be useful for comparison.
Conflict of InterestsThe authors state that they have no conflict of interests.
Please cite this article as: Arias SJ, Neffen H, Bossio JC, Calabrese CA, Videla AJ, Armando GA, et al. Prevalencia y características clínicas del asma en adultos jóvenes en zonas urbanas de Argentina. Arch Bronconeumol. 2018;54:134–139.







