


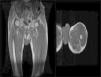
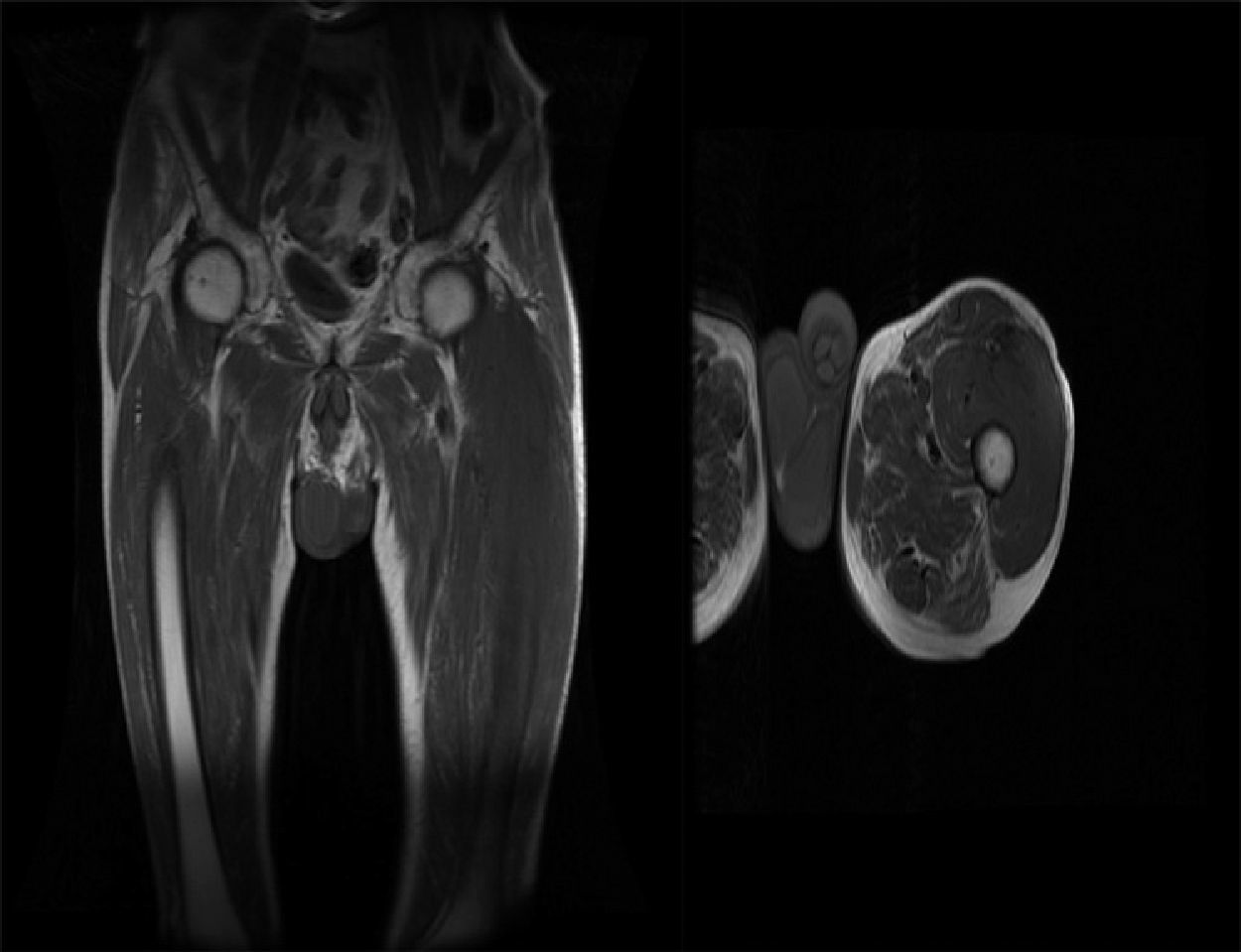
We report the case of a 60-year-old patient, active smoker (40 pack-years), employed in the construction sector. In 2011, he presented in the emergency room with atypical chest pain. Chest X-ray revealed significant pleural effusion, and he was hospitalized. The study was completed with a computed tomography (CT) of the chest and abdomen, which showed bilateral pleural thickening with significant pleural effusion. Positron emission tomography (PET)-CT confirmed bilateral pleural uptake but ruled out pulmonary nodules and other distant involvement. Tumor disease was suspected, so a pleural biopsy was obtained using video-assisted thoracoscopy, and pleural malignant mesothelioma was confirmed. The extension of the lesion rendered it inoperable, and the patient was referred to medical oncology. Here, we began first-line treatment with a platinum and pemetrexed doublet, and partial response according to RECIST criteria was recorded after 4 cycles, with reduction of the pleural implants and effusion, and low toxicity. Given the clear clinical benefit, treatment continued with single-agent pemetrexed as maintenance therapy with radiological follow-up every 3 months.1 The disease remained stable with optimal oncological control for 2.5 years, when the patient developed pain in the region of the left thigh. Examination revealed increased consistency in the area, which was hard and painful on palpation. A magnetic resonance imaging study performed to rule out a neoplastic process in this region showed a soft tissue lesion involving the whole of the thigh, extending to the gluteus. Radiological characteristics were consistent with secondary involvement (Fig. 1). Given the rarity of the observation, an ultrasound-guided biopsy was performed, confirming metastatic malignant mesothelioma. In view of our patient's prolonged oligometastatic disease, local radiation therapy to the muscle lesion was proposed. Moreover, because he was clearly benefitting from systemic treatment and in view of the lack of second-line options, he continued the same therapeutic regimen with oncological monitoring for another 12 months.
Our case is an example of the clinical and therapeutic management of long-term pleural malignant mesothelioma which raises 2 points of interest: prolonged survival achieved with the treatment, and the presence of secondary musculoskeletal involvement. Malignant mesothelioma is a rare tumor that is characterized by involvement of the serous membranes, most commonly the pleura. It is traditionally associated with exposure to asbestos, although other risk factors have been identified.2,3 The initial clinical presentation is characterized by pleuritic pain and pleural effusion. Diagnosis is difficult, and depends in many cases on ruling out other entities. Pleural biopsy is required for a definitive diagnosis.1 Most newly diagnosed pleural mesothelioma cannot be treated locally, and require systemic treatment with chemotherapy, but this tumor is largely chemo-resistant, and therapeutic options are limited. Indeed, consistent data are only available on first-line treatment, and options after progression are currently unclear.1,4 Despite this being a highly aggressive tumor, dissemination is generally local, and symptoms caused by compression and direct invasion cause the patient to deteriorate rapidly. Distant dissemination, as observed in our patient, is much more uncommon, and the development of musculoskeletal metastasis despite control of the pulmonary disease is exceptional. These events suggest that long-term tumors might disseminate atypically to the so-called “sanctuary organs”, where the tumor can evade oncological control. More food for thought is that in oligometastatic patients, continuing systemic treatment while adding a local treatment appears to be a valid therapeutic option.
Our case illustrates a pleural mesothelioma with an atypical course: unusual features include the patient's long survival on oncological treatment (36 months, when mean survival is around 12 months), and an exceptionally rare site of dissemination.
Please cite this article as: Cruz Castellanos P, González Merino T, de Castro Carpeño J. Afectación muscular de un mesotelioma maligno pleural de larga evolución. Arch Bronconeumol. 2018;54:284–285.







