



We report the case of patient who underwent an upper gastrointestinal endoscopic procedure 16 years previously. She presented with a clinical picture of repeated pneumonia, chronic cough, and a sensation of intrathoracic drip when lying on her right side. Chest computed tomography was performed, showing a bronchoesophageal fistula (BEF) in the right intermediate bronchus and extensive bilateral pulmonary consolidation with bronchiectasis due to repeated episodes of aspiration (Fig. 1). Findings were confirmed with bronchoscopy and gastroscopy. The BEF was repaired surgically with lower and middle bilobectomy.
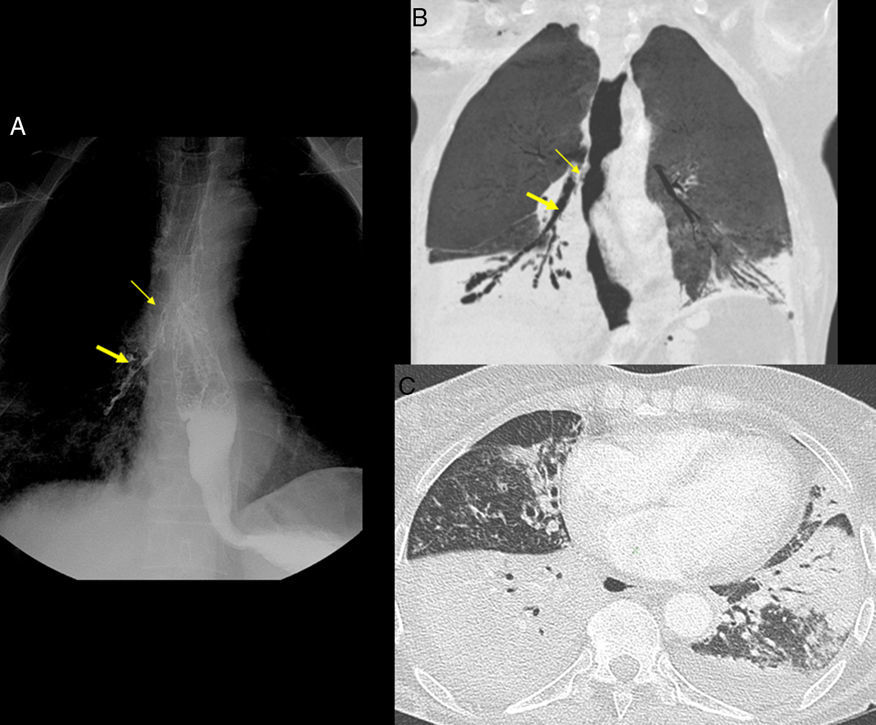
(A) Esophagogram with iodinated oral contrast medium, showing the passage of contrast through the fistula (thin arrow) from the esophagus to the right intermediate bronchus (thick arrow). (B) Chest CT, minIP coronal reconstruction, showing the fistula (thin arrow) from the esophageal lumen to the right intermediate bronchus (thick arrow). Consolidations can also be seen in both lower lobes. (C) Chest CT, axial reconstruction, pulmonary parenchyma window. Due to multiple previous episodes of aspirations, the patient had bilateral pneumonia. Pulmonary consolidation was observed in the middle and lower lobes with some degree of bronchiectasis in the middle lobe.
BEFs can be congenital or acquired. Acquired BEFs are caused by both malignant and benign disease. The most common malignant cause is esophageal cancer. Benign causes may be infection, including tuberculosis, syphilis, and histoplasmosis; trauma, including prolonged endotracheal intubation, closed chest injury or ingestion of a foreign body; or inflammation, including Crohn's disease and Behçet's disease. Endoscopic procedures rarely cause BEF.
Treatment may be interventional or surgical. Interventional treatment may be stent placement in the esophagus or the bronchus, closure with biological glue, or electrocoagulation. Surgery includes fistula repair, fistula closure with muscle or omental flap, and esophageal bypass with resection of the fistula.1,2
Please cite this article as: Fernández Gajardo J, Gómez Herrero H, Viteri Ramírez G. Fístula broncoesofágica adquirida de larga evolución. Arch Bronconeumol. 2018;54:283.







