



We read with great interest the recent article from Crespo-Lessmann and Torrego-Fernández in which they present a patient with obstructive inflammatory tracheal pseudomembrane (in the form of a tracheal septum) secondary to repeated endotracheal intubations. In their article, the authors describe the complete resolution of the process with respiratory physiotherapy and the administration of anti-inflammatories (glucocorticoids).1
Obstructive fibrinous pseudomembrane is a rare condition, but probably more common than reported in the literature. It originates from ischemia of the tracheal mucosa, usually due to iatrogenesis, inducing the production of growth factors and abnormal regeneration.2 This results in the formation of a fibrous membrane that partially obliterates, and in some cases, even totally obstructs the tracheal lumen.3 As the authors indicate, these acquired inflammatory lesions can resolve spontaneously after a certain length of time. However, the central airway is frequently compromised and urgent endotracheal intervention is required.
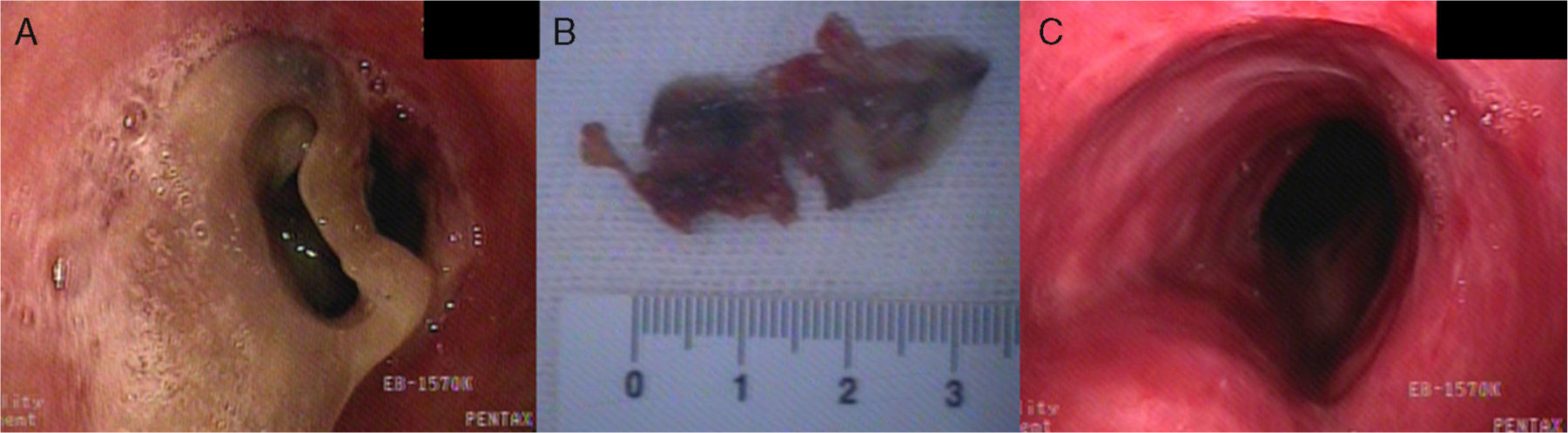
We report here our experience with a 69-year-old male non-smoker who had undergone surgery for herniated disc in the lumbar spine, requiring general anesthesia and orotracheal intubation. The procedure was carried out with the patient in the prone position, thus increasing endotracheal tube cuff pressure. During the immediate post-surgical period, the patient suffered respiratory arrest and was reintubated. A flexible bronchoscopy was performed, revealing a partially detached circumferential fibrinous pseudomembrane causing stenosis of the entire upper third of the tracheal lumen (Fig. 1A). A fragment of approximately 2cm that was acting as a valve and may have caused the patient's respiratory arrest was removed with the biopsy forceps during the same procedure. To gain better control of the airway after extraction of the pseudomembrane a rigid bronchoscopy was performed, during which the tracheal lesion was extracted en bloc using the bevel of the tracheoscope (EFER-DUMON® caliber 14mm) (Fig. 1B). The patient subsequently progressed favorably and could be extubated a few hours later (Fig. 1C). In the case presented by Crespo-Lessmann and Torrego-Fernández,1 the tracheal septum may have originally been a fragment of circumferential pseudomembrane. In their case, the evolving nature of the condition and the clinical picture could have permitted conservative treatment.
Obstructive tracheal pseudomembrane, therefore, must be diagnosed with endoscopy as soon as possible after clinical suspicion has been aroused. Endoscopic monitoring would be advisable in patients who have required prolonged or repeated endotracheal intubations. Since severe respiratory complications are common, therapeutic endoscopy is required in the majority of the cases reported in the literature.4,5 A conservative approach is only an option in carefully selected patients, and even these patients must be very closely monitored (Fig. 1).
Please cite this article as: Arenas-de Larriva MS, Cosano-Povedano J, Cosano-Povedano A. Seudomembrana traqueal inflamatoria. Arch Bronconeumol. 2014;50:307–308.







