



Pulmonary artery agenesis is a rare disease with a prevalence of 1 in 200000 adults. It is associated with cardiovascular abnormalities, and is diagnosed in childhood. Patients can sometimes remain asymptomatic until adulthood without experiencing other complications.
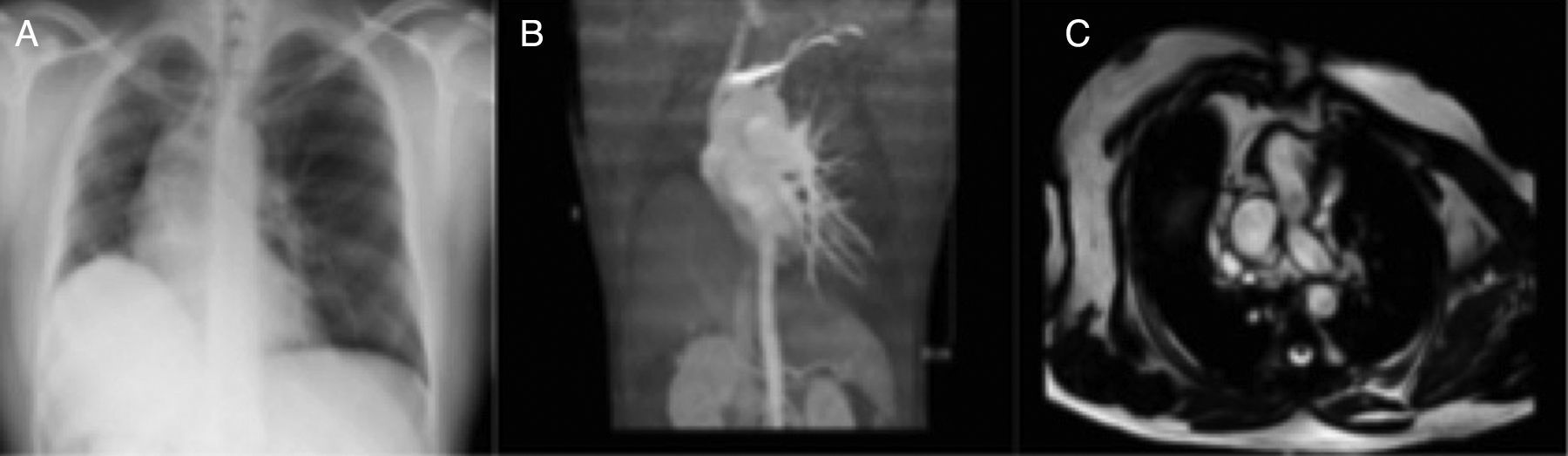
We report the case of a 47-year-old man, referred to the pulmonology clinic after observation of elevated right hemidiaphragm on a routine chest X-ray (Fig. 1). The patient was a former smoker with no other history of interest. He did not report any symptoms.
Thoracic ultrasound was requested, which revealed an elevated right hemidiaphragm, with no signs of paradoxical movement.
Chest computed tomography (CT) (Fig. 1) showed findings consistent with right pulmonary artery agenesis, and an underdeveloped right lung with compensatory eventration of the contralateral lung. The examination was completed with cardiac magnetic resonance imaging (Fig. 1), which showed right pulmonary artery agenesis and partial agenesis of the right lung. The right upper lobe was draining via a single right pulmonary vein to the left atrium, with no evidence of an artery feeding that lobe, nor of shunts or other anomalies. Pulmonary hypertension was ruled out by echocardiogram.
Since the patient was asymptomatic, we decided to treat him conservatively with clinical follow-up in the pulmonology clinic.
Unilateral pulmonary artery agenesis is a rare congenital anomaly, caused by an anomaly in the rotation and migration of the sixth primitive aortic arch in the fourth or fifth week of embryonic development. Absent pulmonary artery is more frequent in the right branch than in the left. It is classified into three groups, depending on the clinical presentation1: in group I, a left-to-right shunt develops and is diagnosed in childhood. In group II, severe pulmonary hypertension occurs and these patients generally die in the first few months of life. Group III consists of adults with few manifestations. The most common symptoms in adults are dyspnea, chest pain, hemoptysis, and recurrent infections, and 44% of patients develop pulmonary hypertension.2
This disease is generally diagnosed in childhood, in association with other cardiovascular malformations. A diagnostic suspicion in adulthood can be prompted by an abnormal chest X-ray.3 The definitive diagnostic test is CT with contrast medium and/or magnetic resonance imaging and/or angiographic studies.
There is no consensus on treatment. Some authors have recommended the use of repeated echocardiograms to monitor the development of pulmonary hypertension.4 In these cases, treatment with specific vasodilators or revascularization of the affected lung can improve patient progress.5 When lung infections are recurrent or severe hemoptysis develops, lobectomy or pneumonectomy is indicated.
Pulmonary artery agenesis, though rare, should be considered in the differential diagnosis of adults with recurrent lung infections or hemoptysis. Chest X-ray is a useful tool for the initial diagnosis, which should be confirmed by CT scans with contrast medium or magnetic resonance imaging.
We thank the Respiratory Medicine Department of the Hospital Universitario Virgen de la Victoria, and, in particular, Dr. Juan Antonio Romero Arias.
Please cite this article as: César EC, Aguirre MCF, Jiménez LP. Hallazgo incidental de agenesia de la arteria pulmonar derecha en el adulto. Arch Bronconeumol. 2017;53:693–694.







