




Endobronchial lipoma is a rare benign neoplasm of the tracheobronchial tree. Despite its benign nature, associated endoluminal polypoid growth can cause bronchial occlusion. In this paper, we present the consequences of a late diagnosis of this condition.
El lipoma endobronquial es una neoplasia benigna del árbol traqueobronquial poco frecuente. A pesar de su naturaleza benigna, puede producir la oclusión bronquial, debido a su crecimiento polipoide endoluminal. En este artículo se presentan las consecuencias de un diagnóstico tardío en este tipo de lesiones.
Benign neoplasms of the tracheobronchial tree are rare. Endobronchial lipoma is a benign tumour with an incidence of 0.1%–0.5% of all lung neoplasms. It originates from the cells of the peribronchial adipose tissue and, occasionally, from the sub-mucosal tissue of the main bronchus. Clinical symptoms depend on its location, degree of bronchial obstruction and morphological and functional consequences of the obstruction on the distal parenchyma. Thus, early diagnosis and radical treatment are essential in order to avoid irreversible pulmonary lesions. We present the case of a 63-year-old man with endobronchial lipoma, who underwent anatomical lung resection due to his late diagnosis.
Clinical CaseThe patient was a 63-year-old man, ex-smoker for 36 years (40 pack-years), with a history of bronchial asthma. He had symptoms of a dry cough and intermittent dyspnoea, and was being monitored in the Respiratory Medicine department for bronchiectasis. A routine computed tomography (CT) scan for his respiratory disease highlighted the presence of an endobronchial lesion in the left lower lobe (Fig. 1A). Fibrobronchoscopy was subsequently performed, showing an endoluminal lesion in the lower bronchus. No malignant neoplastic signs were detected in either the biopsy or cytology, despite repeating these studies on a further two occasions. In view of these findings and the absence of symptoms, it was decided to maintain clinical and radiological follow-up. In the last few months, he had episodes of haemoptysis and persistent respiratory infections that improved with antibiotic treatment. New imaging tests (Fig. 1B) and an endoscopic examination (Fig. 1C) revealed an increase in the size of the polypoid lesion extending towards the left main bronchus, more than 2cm from the main carina. Acute inflammatory changes were also observed on this occasion, both in the bronchial aspirate and in the bronchial biopsy, with no neoplastic cells detected.
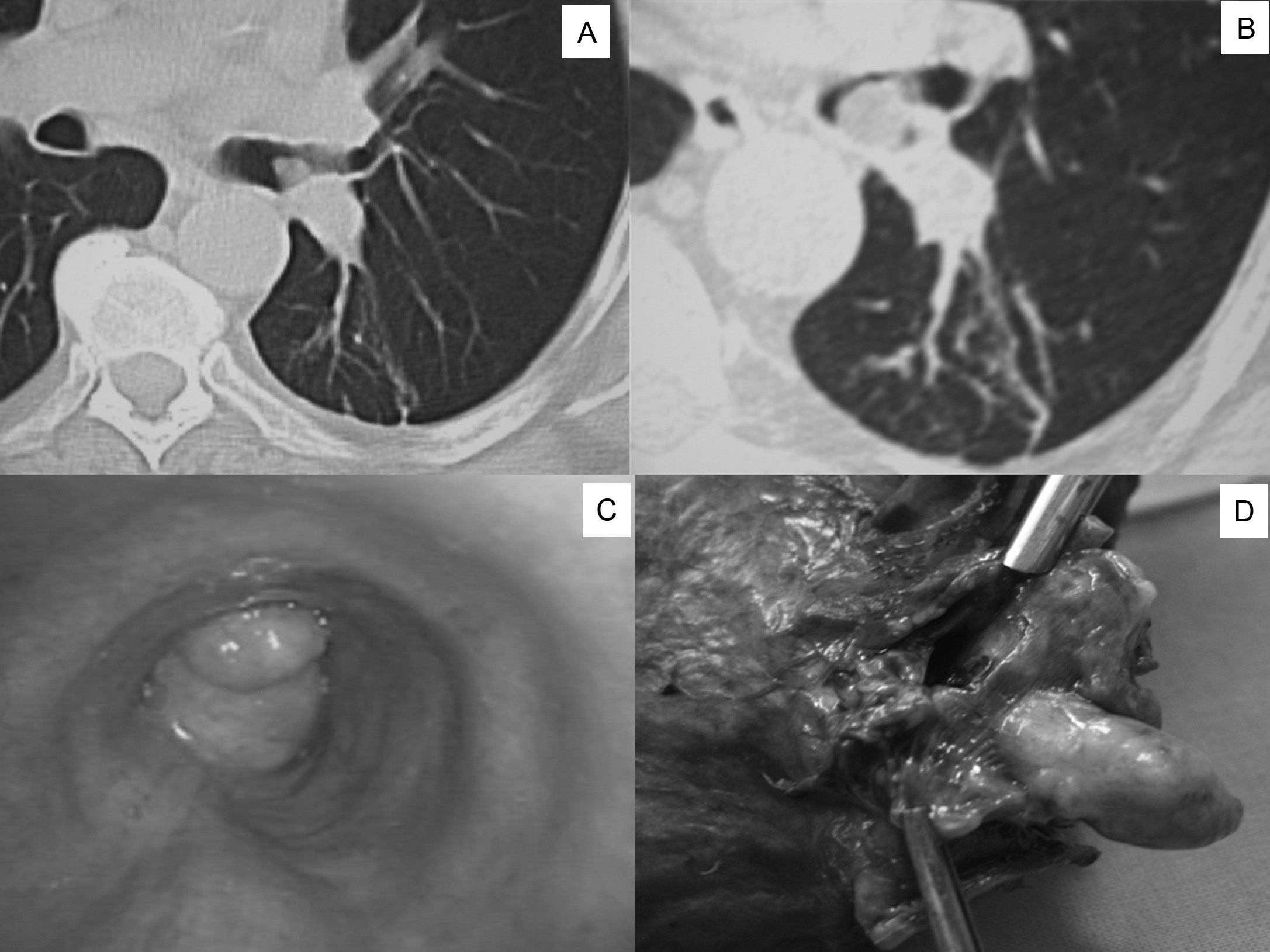
(A) An endobronchial lesion can be observed in the left lower lobe at the level of the interlobar carina on the chest CT scan. (B) Chest CT scan one year later: growth of the endobronchial lesion towards the lumen of the main bronchus can be seen. (C) Fibrobronchoscopy: endobronchial lesion protruding towards and partially occluding the lumen of the main bronchus. (D) Surgical specimen: polypoid lesion originating from the lower lobe bronchus.
Due to the suspicion of a malignant lesion and the difficulty in obtaining a diagnosis, it was decided to operate on the patient. A video thorascopic examination was performed, observing the presence of signs of hepatisation and fibrosis in the lower lobe, as well as the presence of multiple firm adhesions mainly in the costodiaphragmatic recess, which prevented the examination from being completed. A left lower lobectomy was eventually performed by lateral thoracotomy. When the lower bronchus was sectioned, a 2cm yellow pediculated tumour with smooth borders was identified, originating from the walls of the lower lobe bronchus and protruding towards the lumen of the main bronchus (Fig. 1D). The patient did not present any complications during the post-operative period and was discharged on the fifth day.
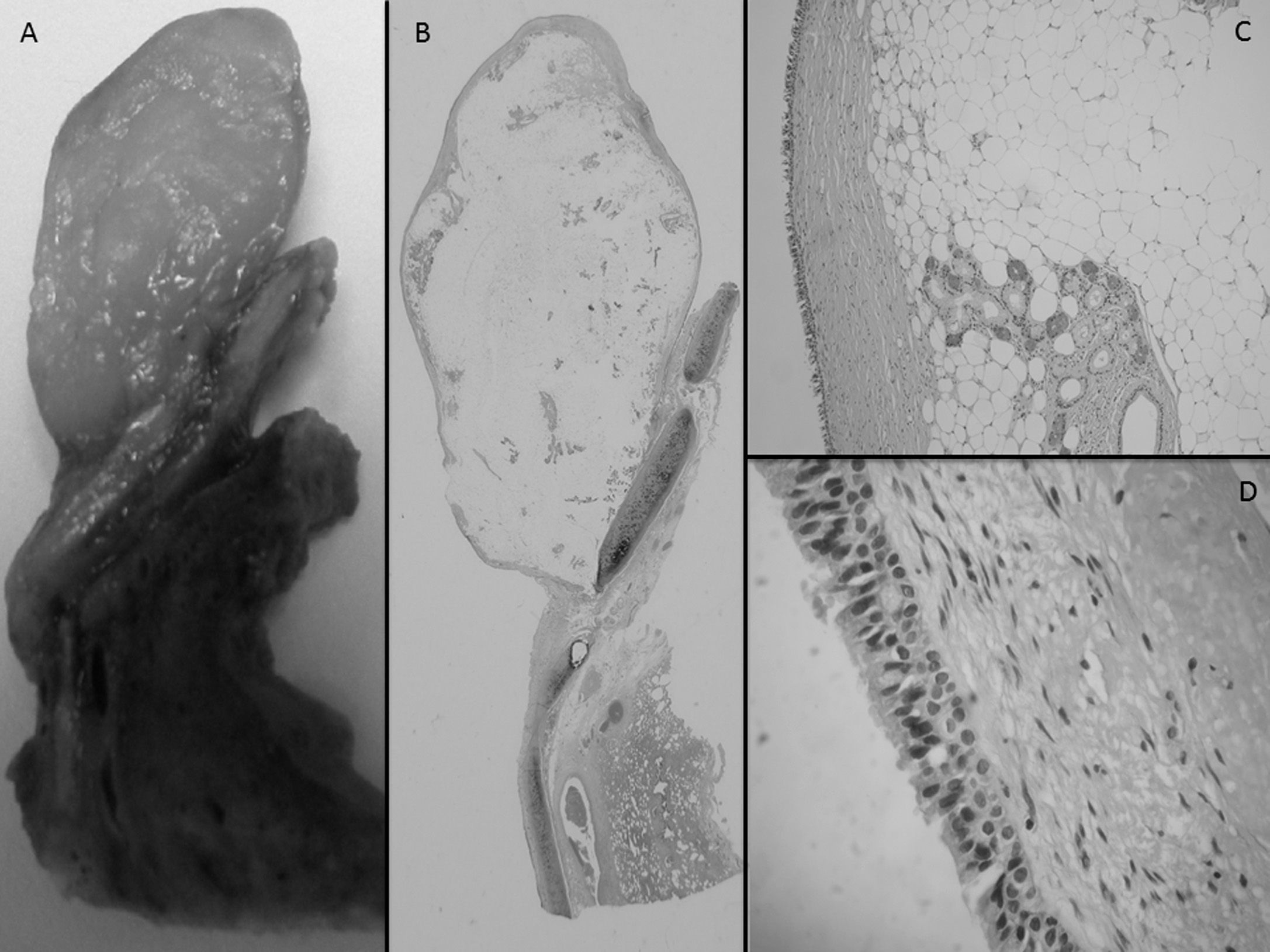
The pathology study revealed the lesion to be a benign mesenchymal neoplasm made up of mature adipose tissue surrounding bronchial glandular structures. In view of these findings, a diagnosis of endobronchial lipoma was made.
DiscussionEndobronchial lipomas are extremely rare benign lung tumours that represent 0.1%–0.5% of all lung neoplasms.1 They are more common in men, with a peak incidence between the fifth and sixth decades of life. Obesity and smoking are considered risk factors, although there are no conclusive studies. Endothoracic lipomas can be classified into 5 groups: cardiac, parenchymatous, pleural, mediastinal and endobronchial, as in our case. In most cases described in the literature, the tumour is located in the first three subdivisions of the tracheobronchial tree, and is more common on the right side, although in our case, it originated in the left lower lobe bronchus.1,3
Cough, progressive dyspnoea, haemoptysis and recurrent pneumonia are the most common forms of presentation. These patients can sometimes be erroneously diagnosed with bronchial asthma, delaying the diagnosis of these types of lesions.4,5 Fibrobronchoscopy is the fundamental tool for its diagnosis, enabling the lesion to be located and biopsied,4,5 although in our case the samples obtained were unrepresentative (Fig. 2).
Despite their benign nature, their growth can cause partial or total obstruction of the bronchus, as well as destruction of the distal parenchyma.5 Bronchoscopic resection should be considered as the first therapeutic option, as it avoids both thoracotomy and lung resection, with the resulting functional impact that this entails. However, if there are irreversible changes in the parenchyma, such as fibrosis, pneumonia or atelectasis, lung resection must be performed.2,4,5 In our case, the presence of said findings, due to the late diagnosis, did not allow endoscopic resection to be carried out, and a lower lobectomy was necessary.
Please cite this article as: Triviño A, Mora-Cabezas M, Vallejo-Benitez A, García-Escudero A, González-Cámpora R. Lipoma endobronquial: una causa poco frecuente de obstrucción bronquial. Arch Bronconeumol. 2013;49:494–496.







