



SARS-CoV-2 disease (Covid-19) is an infection caused by a new emerging coronavirus first detected in Wuhan, China, in December 2019. It has now become a pandemic and is posing a serious public health problem for almost all countries.1 In particular, the incidental diagnosis of thoracic tumors in patients with SARS-CoV-2 infection represents an additional challenge, both from a diagnostic and therapeutic point of view. Some publications have addressed the clinical management of cancer patients in the current SARS-CoV-2 pandemic, but there are no specific guidelines for performing thoracic diagnostic interventional procedures in patients with tumors who are also infected with SARS-CoV-2.2–12 We report two cases in which thoracic tumors were detected that required biopsy with radiological control at the peak of the Covid-19 pandemic that hit Madrid in the second half of March 2020.
These were 2 patients (a 19-year-old woman with no history of interest, and a 73-year-old man, former smoker) who came to our hospital with chest symptoms (fever, cough, and dyspnea) in the second half of March 2020, coinciding with the peak of the Covid-19 pandemic that struck Spain and, in particular, the Madrid region. Both patients underwent polymerase chain reaction (PCR) testing for SARS-CoV-2 and a chest X-ray in the emergency department. In both cases PCR was positive and chest X-ray showed opacities of infectious appearance and a tumor mass. Treatment for SARS-CoV-2 infection was started in both patients (with good clinical progress) and a CT scan of the chest was performed, confirming the tumor lesions. The 19-year-old patient had a voluminous mass in the right hemitorax with destruction of the third costal arch and invasion of the chest wall and spinal canal. Ipsilateral pleural implants of metastatic appearance and some ground glass opacities of an infectious nature were also observed in the right lung base (Fig. 1A–D). The 73-year-old patient had a 6 cm mass in the upper right lobe, adenopathies in the ipsilateral pulmonary hilum, and bilateral opacities of pneumonic appearance (Fig. 1E–G). In this second case, no signs of distant metastases were observed. During the fortnight in which the two patients were admitted (March 16–31, 2020), the region of Madrid endured the highest number of cases and deaths from this pandemic in the whole country, and our center, a university hospital in Madrid with about 850 beds, had virtually become a “Covid-19 dedicated” center, with more than 950 patients admitted with SARS-CoV-2 infection. Because of this situation, most of the hospital’s clinical activity (like many other centers throughout the country) was focused on the treatment of Covid-19 patients, and large numbers of medical personnel (including pulmonologists, medical oncologists and radiation therapists, thoracic surgeons, pathologists, and radiologists) had been recruited from different departments of the center for the care and management of these patients. As a result of this unusual situation, most of the hospital's “ordinary” clinical activity was suspended, including the routine care of cancer patients (consultations, day hospital, radiotherapy sessions, follow-up radiological studies). However, in the case of our 2 patients, we decided to perform a CT-guided biopsy of the lesions in the hope of obtaining an early histological diagnosis and being able to start specific treatment as soon as possible. Because both patients had Covid-19, the biopsy procedure was performed on the CT equipment of our hospital reserved for patients with this infection. During the procedure, the infection control protocol of the radiodiagnostics department was followed and personal protective equipment (PPE) was used. Both patients wore masks, while radiology staff who participated in the biopsy procedure followed our hospital’s Covid-19 control protocol and used PPE, since core needle biopsy is considered a potentially aerosol-generating procedure.13 PPE included gloves, FFP2 filter mask, goggles, face shields, robe, aprons, cap and shoe coverings. At the end of the biopsy procedures we followed our hospital’s protocol for decontaminating the CT scanner. Histologic diagnosis confirmed Ewing's sarcoma of the chest wall in the 19-year-old patient and pulmonary adenocarcinoma in the 73-year-old patient, and treatment was started after discussion of both cases by the thoracic tumor multidisciplinary committee (virtually via teleconference).
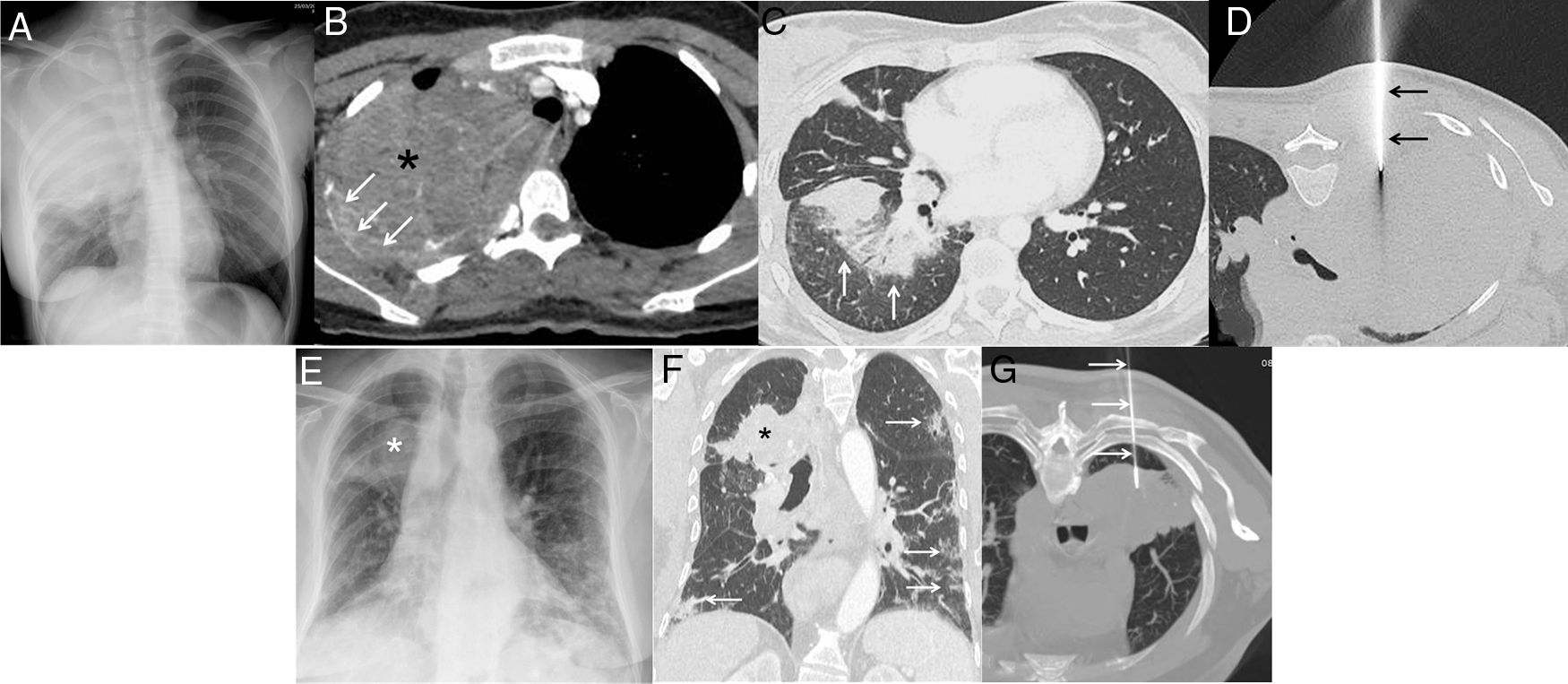
A–D) A 19-year-old patient with dyspnea, chest pain, cough, and fever. A) Posteroanterior chest X-ray showing a large mass in the right hemitorax and partial destruction of the right third costal arch. B) Axial CT image of the chest (mediastinum window) confirming a large heterogeneous mass in the right hemitorax (asterisk) with destruction of the right third costal arch (arrows). C) Axial CT image of chest (lung window) showing peri-bronchial ground glass opacities of infectious appearance (arrows). D) Axial CT image of chest (patient in prone position) during biopsy procedure (arrows mark biopsy needle). E–G) A 73-year-old patient with fever, cough, and dyspnea. E) A posteroanterior chest X-ray showing a mass in left upper hemitorax (asterisk) and bilateral opacities of an infectious appearance. F) Chest CT coronal image (lung window) showing lung mass (asterisk) and bilateral pneumonic opacities (arrows). D) Axial CT image of chest (patient in prone position) during biopsy procedure (arrows mark biopsy needle).
As cases of Covid-19 escalate exponentially throughout the world, saturating hospitals and accounting for more than 200,000 deaths worldwide (as of April 25, 2020), many institutions have had to prepare themselves to deal with the avalanche of patients with SARS-CoV-2 infection. At our center, this preparation included the secondment of the majority of hospital staff to care for the more than 950 patients in newly created “Covid-19 units”. In this scenario, only oncological emergencies and critically ill cancer patients were being treated in the hospital, while the vast majority of outpatient visits and diagnostic procedures were postponed. The proper clinical management and safety of cancer patients (both patients in follow-up and newly diagnosed cases) in the current Covid-19 pandemic should be a priority and each institution should establish contingency plans.2–12 Some authors have suggested postponing adjuvant chemotherapy or elective surgery in patients with less aggressive tumors, reducing the frequency of hospital visits for cancer patients, and developing appropriate isolation protocols to mitigate the risk of SARS-CoV-2 infection in these patients.14 Other authors have proposed that more intensive surveillance or treatment should be considered for cancer patients who also have COVID-19.15 Recent articles have reminded us how important it is for radiology departments to be prepared for COVID-19 (from the indication of chest X-rays or CT to the protection of their staff),16 but there are no specific guidelines for performing diagnostic thoracic interventional procedures in patients with tumor lesions who are also infected with SARS-CoV-2.
The purpose of this report is to send a clear and positive key message that image-guided chest biopsies in cancer patients who are also infected with SARS-CoV-2 are feasible and safe (even at the height of the pandemic), provided that appropriate safety measures are taken by the health personnel involved in the procedure. We believe that cancer patients, regardless of whether they are infected with SARS-CoV-2 (and regardless of the phase of the pandemic), continue to deserve our dedication and care.
Please cite this article as: Gorospe L, Ayala-Carbonero AM, Ureña-Vacas A, Medina-Díaz M, Arrieta P, Mirambeaux-Villalona RM, et al. COVID-19: intervencionismo diagnóstico torácico en tiempos difíciles. Arch Bronconeumol. 2020;56:674–676.







