
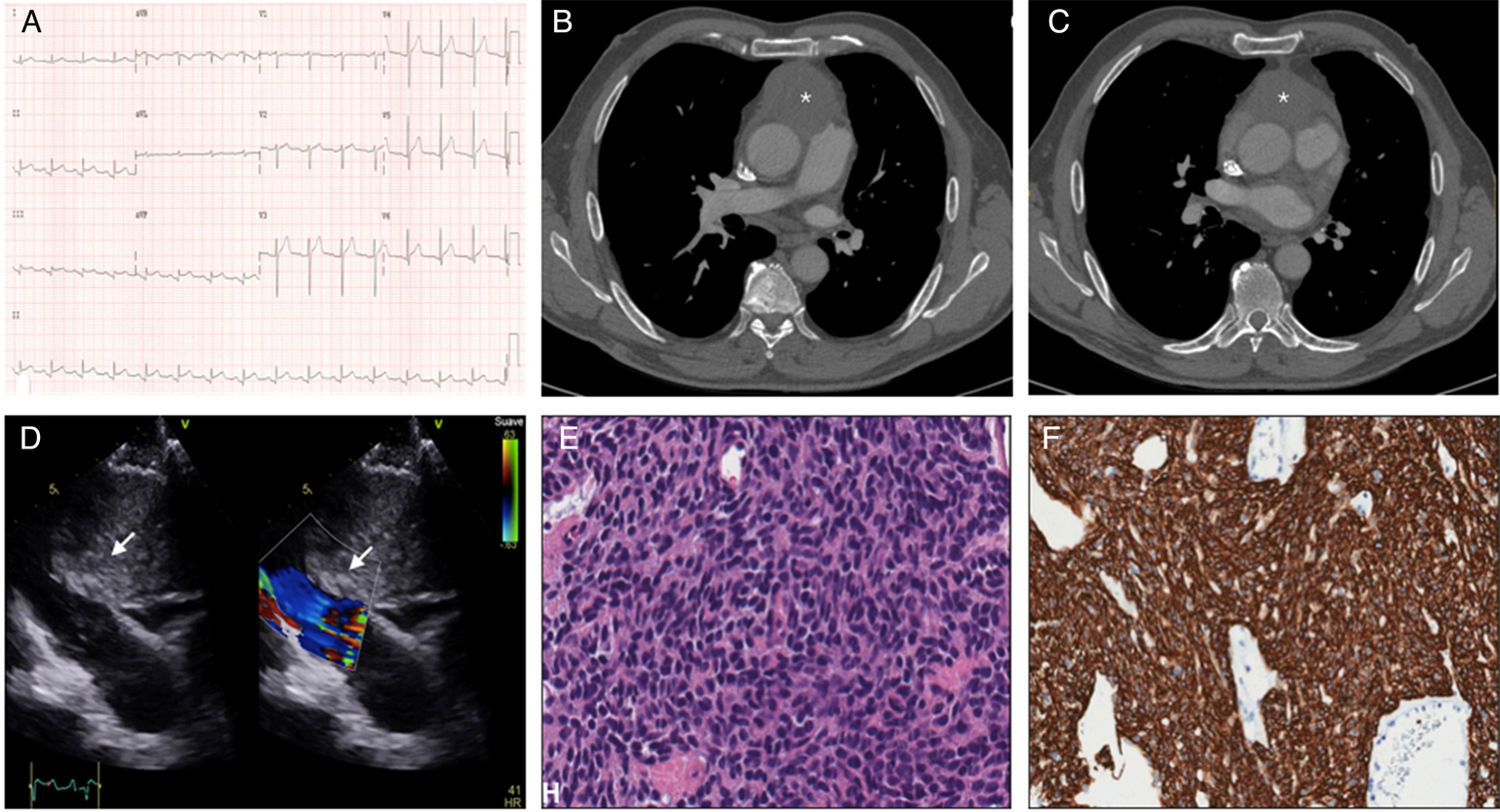
A 71-year-old man with no significant history presented with central chest pain. Electrocardiogram showed ST segment elevation in the lower leads, so code STEMI was activated (Fig. 1A), but emergency coronary catheterization revealed no coronary lesions. Chest X-ray showed no findings of interest and clinical laboratory tests showed D-dimer 650ng/ml, so chest angio-CT was performed, revealing a mass in the anterior mediastinum (Fig. 1B and C). The echocardiogram showed mild pericardial effusion impinging on the pericardium. The tumor was also compressing the right ventricular outflow tract and the pulmonary artery (Fig. 1D). Core needle biopsy was performed, revealing neoplastic epithelial cells positive for CK5/6 and CKAE1/AE3, consistent with type A thymoma (Fig. 1E and F). The surgical option of tumor resection and revascularization by aorto-coronary bypass was considered, but was ruled out given the significant pericardial invasion, so radiation and chemotherapy were started.
Malignant thymoma is the most common tumor of the anterior mediastinum, and although it can cause chest pain, other cardiovascular manifestations are rare.1 The proximity and invasion of cardiac structures can cause coronary compression, pericarditis, pericardial tamponade, hemodynamic obstruction (as in our case), or superior vena cava syndrome.2
Please cite this article as: Piqueras-Flores J, Rayo-Gutiérrez M, de Lara-Simón IM. Síndrome coronario como primera manifestación de timoma invasivo. Arch Bronconeumol. 2018;54:40.







