

Platypnea-orthodeoxia syndrome (POS) is characterized by onset or worsening of hypoxemia in the upright position which improves or disappears when the patient lies down.1 It is often accompanied by dyspnea. This syndrome is usually caused by a patent foramen ovale, pulmonary intravascular shunt or severe ventilation/perfusion disorders. We report 5 rare cases of POS of cardiac origin in elderly patients, associated with patent foramen ovale which was probably undetected until an intercurrent episode (abdominal surgery or aortic elongation) prompted the manifestation of clinical signs and symptoms. Development of the syndrome can be gradual, over a period of years, or relatively acute, in a matter of months.
All our patients were over 70 years of age (Table 1) with no significant medical history, with the exception of 1 patient who had had a cerebrovascular accident (CVA) 2 years previously, and another who had recently undergone abdominal surgery. All 5 patients presented due to recent appearance of dyspnea. Their physical examination and clinical laboratory results were normal, with the exception of hypoxemia when standing, observed in all 5 individuals. Computed tomography with contrast medium (angio-CT) did not reveal any arteriovenous malformations, embolisms, or changes in pulmonary parenchyma. Cardiac silhouette was normal, and in 4 patients, marked dilation of the ascending and descending aorta was observed. Initial transthoracic echocardiography without contrast showed subtle changes that could be appreciated once the diagnosis was known. Respiratory function tests, including carbon monoxide diffusion (DLCO), were normal. Once the association between hypoxemia and desaturation and the patient's position had been established − in 1 patient SpO2 shifted from 93% in a standing position to 62% in a sitting position (Table 1) − transesophageal echocardiograms were performed with the administration of agitated saline contrast (Fig. 1). This procedure revealed patent foramen ovale in all patients, with aneurysm of the interatrial septum and massive early passage of microbubbles to the left atrium during orthostatism, which diminished when the patient lay down. After the diagnosis was confirmed, antiplatelet treatment with aspirin and percutaneous closure of the patent foramen ovale were indicated. The percutaneous procedure could be performed in 3 patients, but 1 patient required surgical closure and another died suddenly while awaiting intervention. One month after closing the foramen ovale, SpO2 was 96%–98% in a supine position and 97%–98% while seated.
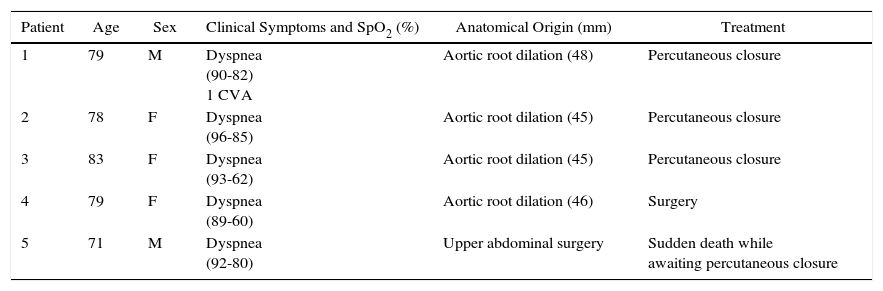
Clinical Details and Treatment of Patients Included in the Series.
| Patient | Age | Sex | Clinical Symptoms and SpO2 (%) | Anatomical Origin (mm) | Treatment |
|---|---|---|---|---|---|
| 1 | 79 | M | Dyspnea (90-82) 1 CVA | Aortic root dilation (48) | Percutaneous closure |
| 2 | 78 | F | Dyspnea (96-85) | Aortic root dilation (45) | Percutaneous closure |
| 3 | 83 | F | Dyspnea (93-62) | Aortic root dilation (45) | Percutaneous closure |
| 4 | 79 | F | Dyspnea (89-60) | Aortic root dilation (46) | Surgery |
| 5 | 71 | M | Dyspnea (92-80) | Upper abdominal surgery | Sudden death while awaiting percutaneous closure |
CVA: cerebrovascular accident; F: female; SpO2: hemoglobin oxygen saturation in a lying position and erect position; M: male.
 Transesophageal echocardiogram with contrast medium (agitated saline) in a lying position, showing passage of few bubbles from the right atrium (AD) to the left atrium (AI) across the patent foramen ovale (black arrow), enhanced by the leftward shift of the intraatrial septum (TIA). (B) Transesophageal echocardiogram with contrast medium performed in a sitting position. The passage of a greater quantity of bubbles is observed, demonstrating the increased right–left shunt. (C) Transthoracic echocardiogram showing marked dilation of the aortic root (Ao), an anatomical condition associated with platypnea-orthodeoxia. (D) Transesophageal echocardiogram showing the patent foramen ovale closure device (white arrow).")
(A) Transesophageal echocardiogram with contrast medium (agitated saline) in a lying position, showing passage of few bubbles from the right atrium (AD) to the left atrium (AI) across the patent foramen ovale (black arrow), enhanced by the leftward shift of the intraatrial septum (TIA). (B) Transesophageal echocardiogram with contrast medium performed in a sitting position. The passage of a greater quantity of bubbles is observed, demonstrating the increased right–left shunt. (C) Transthoracic echocardiogram showing marked dilation of the aortic root (Ao), an anatomical condition associated with platypnea-orthodeoxia. (D) Transesophageal echocardiogram showing the patent foramen ovale closure device (white arrow).
Cardiac POS is an uncommon cause of hypoxemia,2 but one that physicians should be aware of, since it causes hypoxemia symptoms that may be difficult to interpret, and may produce significant sequelae due to paradoxical embolisms associated with ischemic CVAs. Moreover, it is relatively easy to manage, and treatment is usually curative. In our patients, the clinical picture of significant hypoxemia, which we did not initially relate with the patients’ position, and which was not corrected with oxygen, led us to investigate an anatomical shunt and to explore a differential diagnosis between pulmonary vascular malformation (in which the platypnea-orthodeoxia phenomenon can also occur), severe ventilation/perfusion disorder, or intracardiac shunt. After ruling out pulmonary origins with the angio-CT and lung function testing, performed in all patients, the only remaining explanation was an intracardiac shunt. In this syndrome, the shunt may be missed on echocardiogram in decubitus without contrast, so an echocardiogram, preferably transesophageal, with the patient in a sitting position using contrast medium is necessary: this technique clearly shows up massive early passage of microbubbles to the left atrium.3 The sensitivity of the technique may be enhanced by observing the passage of contrast at the end of a Valsalva maneuver. This shunt is the result of a patent foramen ovale with normal pressures in the right cavities, and depending on its anatomical characteristics, can treated with either surgical or percutaneous closure.
Although patent foramen ovale is a congenital heart defect, our patients remained asymptomatic for over 70 years. Patent foramen ovale is normally associated with little or no left–right shunt, so the development of a significant right–left shunt must be due to an acquired abnormality. Cardiac POS can only occur in the presence of an anatomical component, in the form of interatrial communication, and a functional component that causes deformity of the atrial septum, producing a change in the direction of the flow of the shunt when the patient is standing.4 This is observed in patients with patent foramen ovale that is asymptomatic until such time as, generally due to dilation of the ascending aorta, the blood from the inferior vena cava changes direction and flows directly toward the patent foramen ovale (ostium secundum defect) in a standing position, causing displacement of the ostium primum, and allowing the passage of unoxygenated blood into the left atrium.5
Recommended treatment consists of percutaneous closure of the POS, in order to avoid right–left shunt and the subsequent desaturations and dyspnea that occur in an upright position.1 This cannot be achieved with antiplatelet treatment, indicated to prevent CVA in patients with patent foramen ovale and previous ischemic accident.
To conclude, patent foramen ovale is common in the general population and is generally of no clinical consequence. However, it can be associated with paradoxical embolism, CVA and, exceptionally, cardiac POS. It can only be diagnosed if there is a high clinical suspicion in cases of hypoxemia and strange, variable dyspnea. Treatment is generally curative.
Please cite this article as: Sabater Abad C, Juan Samper G, Payá Serrano R, Pérez Boscá JL, Ramón Capilla M, Fernandez Fabrellas E. Síndrome platipnea-ortodeoxia cardiaco: una causa «misteriosa» de hipoxemia. Arch Bronconeumol. 2016;52:494–495.







