

Solitary fibrous tumors of the pleura (SFTP) are rare neoplasms that can spread to different organs. SFTP metastases are usually located in the pleura, chest/abdominal wall, lung, peritoneum and liver; cardiac involvement is exceptional.1,2 We report the case of a patient with an SFTP who developed cardiac metastases.
Our patient was an 87-year-old man, former smoker with a history of anticoagulated atrial fibrillation who underwent surgery for a malignant SFTP. Two years after surgery, a follow-up computed tomography (CT) scan of the chest revealed multiple bilateral pulmonary nodules compatible with metastases (Fig. 1A). CT-guided core needle biopsy confirmed that the pulmonary nodules were consistent with SFTP metastases. In the CT follow-up 1 month later, the pulmonary lesions had grown rapidly, and several nodular lesions were observed in the chambers of the heart, highly suggestive of cardiac metastases (Fig. 1B, C). A few days after the last CT follow-up, the patient was diagnosed with a massive bilateral pulmonary thromboembolism (Fig. 1D) and died a few hours later.
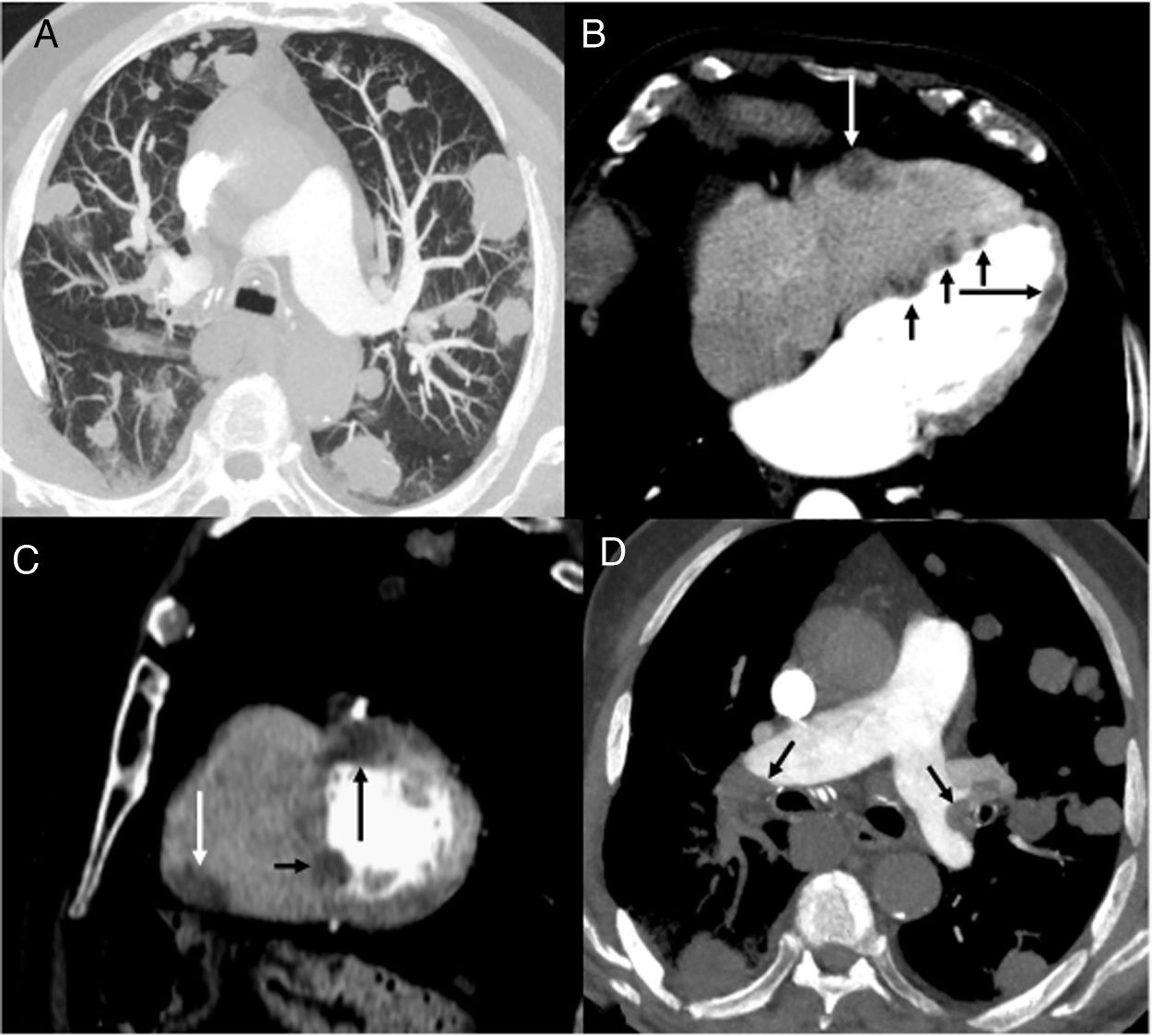
 Axial CT image of the chest (lung parenchyma window), showing multiple bilateral pulmonary nodules. (B and C) Axial (B) and sagittal (C) chest CT images (mediastinal window) showing several nodules in the right ventricular free wall (white arrow), interventricular septum (short black arrows) and left ventricular free wall (long black arrow). (D) Axial CT image of the chest (mediastinum window) showing filling defects in the pulmonary arteries (arrows).")
(A) Axial CT image of the chest (lung parenchyma window), showing multiple bilateral pulmonary nodules. (B and C) Axial (B) and sagittal (C) chest CT images (mediastinal window) showing several nodules in the right ventricular free wall (white arrow), interventricular septum (short black arrows) and left ventricular free wall (long black arrow). (D) Axial CT image of the chest (mediastinum window) showing filling defects in the pulmonary arteries (arrows).
Cardiac metastasis in SFTP is exceptional, and we have only found 1 documented case of left atrium metastasis by intracavitary extension from the left upper pulmonary vein. In our case, the rapid and extensive involvement of several chambers of the heart (coinciding with accelerated pulmonary progression) suggests a previously unreported hematogenous spread of the tumor. Although we were unable to confirm cardiac involvement with histology in our patient, we believe that imaging tests and rapid pulmonary progression (confirmed pathologically) reinforce the hypothesis of a metastatic origin of the cardiac lesions. We also believe that the subsequent pulmonary thromboembolism could be associated with tumor infiltration of the right heart chambers.
FundingThis study did not receive any financial support.
Conflict of interestsThe authors have no conflict of interest to declare.







