



A 45-year-old male former smoker was admitted after receiving bullet wounds to the head and abdomen. On admission, his Glasgow scale score was 3. The patient required immediate intubation in the emergency room, and following emergency laparotomy he was transferred to the intensive care unit (ICU) for respiratory support. Chest computed tomography (CT) did not reveal any signs of chest injury but extensive emphysematous changes with formation of bulla were seen.
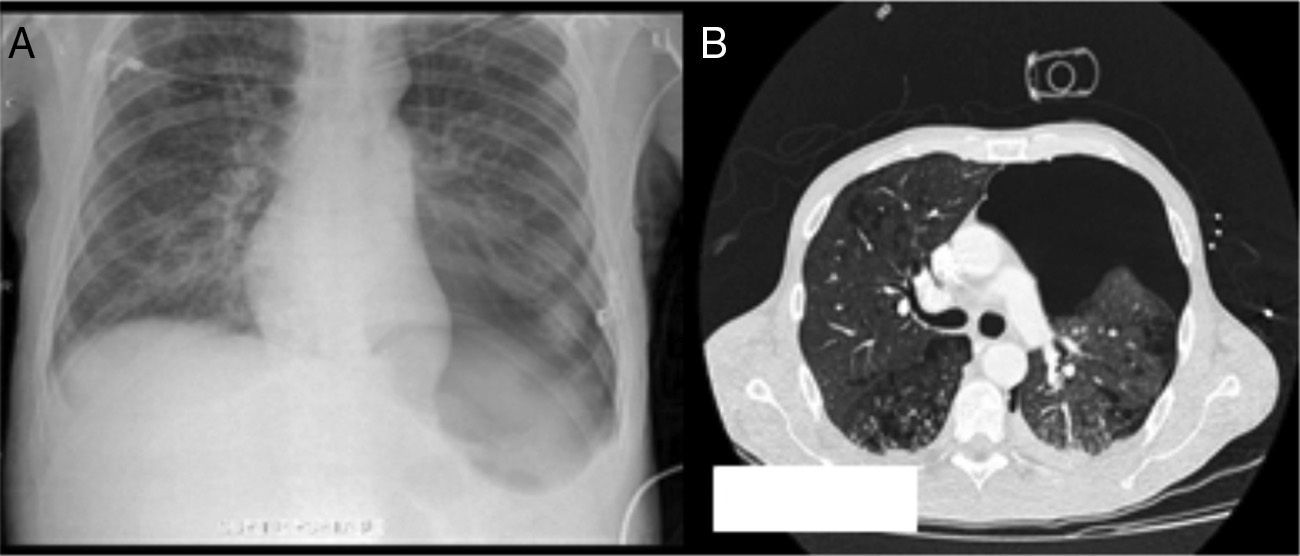
After two weeks of mechanical ventilation in the ICU, a conventional chest X-ray showed hyperlucency (deep sulcus sign) at the base of the left lung, with associated collapse, and depression of the left hemidiaphragm. A pleural line was visible in the apical region of the left lung (Fig. 1A). At that time the patient was asymptomatic and hemodynamically stable. He was receiving volume-controlled ventilation with positive end expiratory pressure (PEEP) of 10cmH2O. Chest CT was performed (Fig. 1B) to complete the evaluation, showing development of a large left pneumothorax that was successfully treated with the insertion of an intercostal chest tube.
To Dr Orla Buckley, Radiologist Consultant in Adelaide and Meath Hospital, Tallaght, Dublin.
Please cite this article as: Chong SG, Moloney E, Fitzpatrick G. Un neumotórax engañoso. Arch Bronconeumol. 2014;50:496.







