



A 42-year-old male farmer presented to our outpatient department with cough, fever and dyspnea. Twenty-five days before admission, the patient had an episode of coughing, during which he expelled about 300ml yellowish material that was salty in taste. Chest computed tomography (CT) revealed a voluminous cavitary lesion in the left upper lobe containing irregular, serpiginous intracavitary material compatible with the free-floating membrane of a hydatid cyst (HC; Fig. 1A–C). Surgical treatment with lobectomy was performed. Dissection of the excised lung revealed a very sharply circumscribed HC measuring about 10cm in diameter (Fig. 1D).
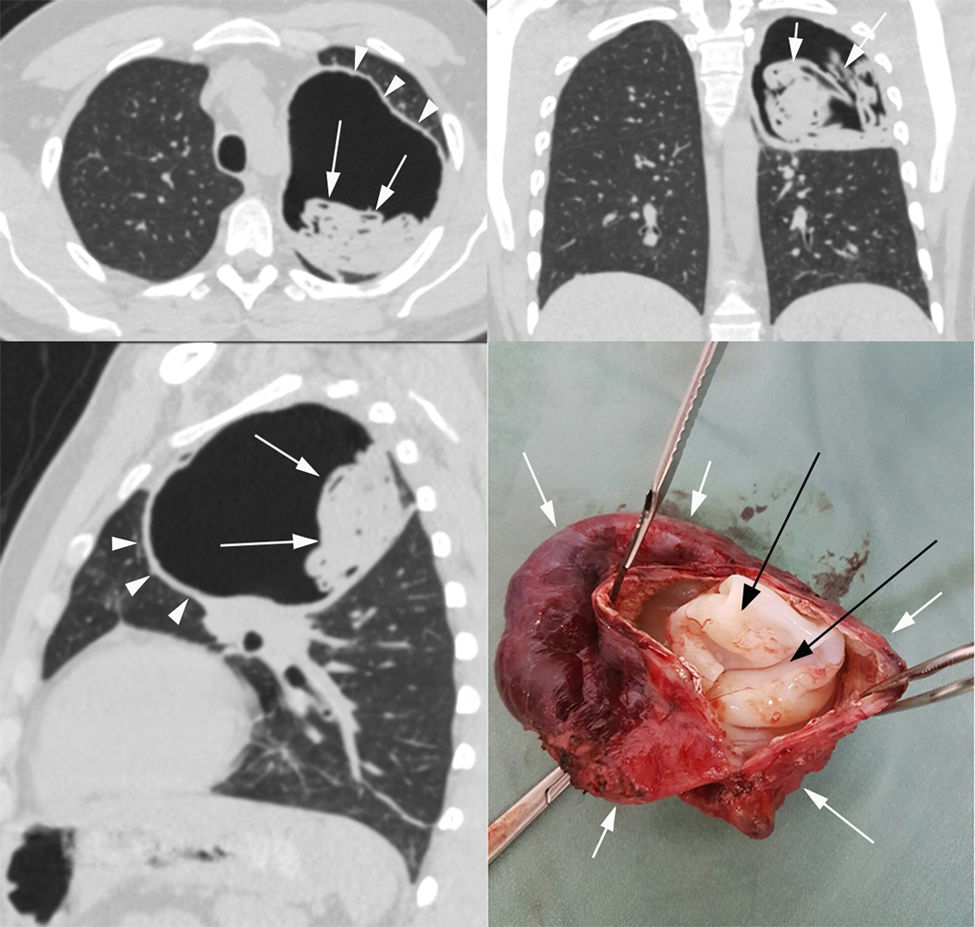
Chest computed tomography with axial (A), coronal (B) and sagittal (C) reconstructions showing a voluminous cavitary lesion (arrowheads) in the left upper lobe containing irregular, serpiginous intracavitary material compatible with free-floating membranes (arrows) of a hydatid cyst (serpent sign). In (D), a photograph of the surgically resected hydatid cyst, showing the outer membrane (pericyst – white arrows) and the inner free-floating membrane (endocyst – black arrows).
In the early stages of the hydatid disease, lung HC generally manifests on CT as a well-demarcated round or oval opacity. When erosion in the adjacent bronchioles occurs, air may enter the space between the endocyst and pericyst, causing detachment or collapse of the parasitic membranes. The collapsed membranes float freely in the cyst fluid, and can present tomographically with different imaging aspects, such as the water lily sign (the membrane floating in the cyst fluid), the air crescent sign (a radiolucent crescent in the upper part of the cyst), and the serpent sign (the collapsed membranes forming serpiginous, twisted structures inside the cyst).1,2 Complications of lung HC include rupture of the cyst, acute pulmonary embolism, anaphylactic reactions, and secondary bacterial infection. Surgery covered or not by perioperative albendazole prophylaxis remains the first-line treatment option for HC.







