
An 83-year-old male with a history of atrioventricular block with a pacemaker presented with small-volume hemoptysis. He had been hospitalized a week earlier with acute dyspnea on exertion and hypoxic respiratory failure, diagnosed with bilateral pulmonary emboli. He underwent suction thrombectomy using an Inari Flowtriever 24 catheter, recovered well, and was discharged on an oral anticoagulant.
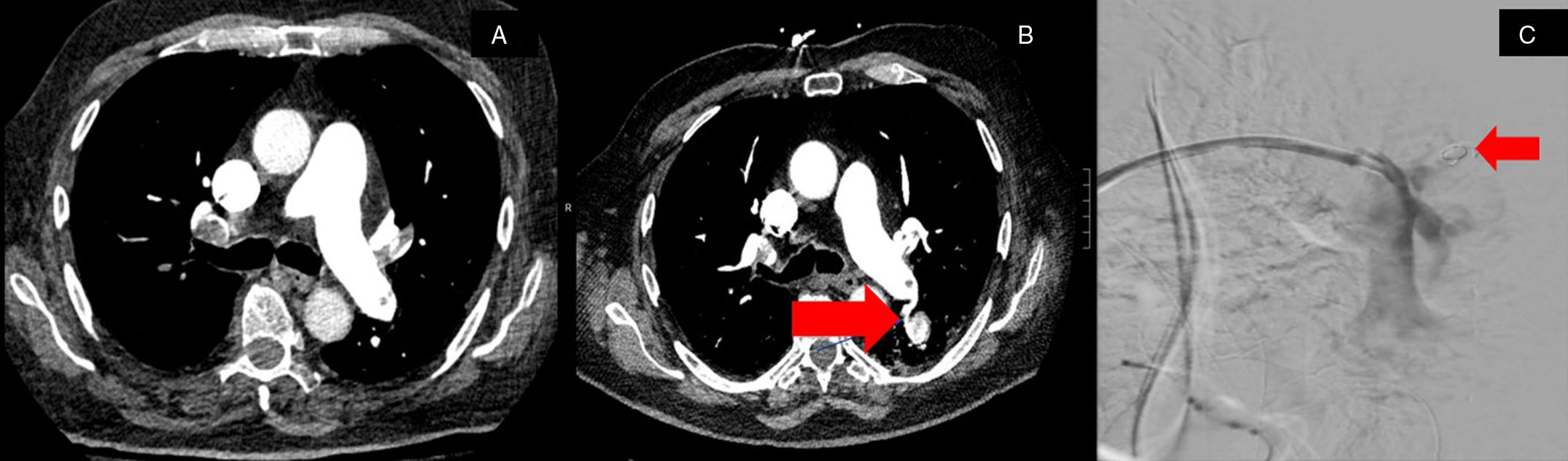
The patient returned to the hospital a day after discharge with hemoptysis, described as a quarter-sized dark red blood clot, occurring about four days post-thrombectomy. A computed tomography (CT) angiogram of the chest compared with the pre-thrombectomy CT chest (Fig. 1A), revealed a significant reduction in pulmonary arterial clot burden. However, a new finding was noted: a heterogeneously hyperdense structure in the superior left lower lobe, appearing connected to a left lower lobe segmental pulmonary artery (Fig. 1B). These findings were consistent with a pulmonary artery pseudoaneurysm. The patient underwent a pulmonary artery arteriogram, which confirmed the presence of the pseudoaneurysm. Following this confirmation, coil embolization was performed, with successful coiling verified fluoroscopically (Fig. 1C). After the procedure, the patient did not experience any recurrent episodes of hemoptysis and recover well.

A – demonstrates a CT image pre-thrombectomy without a pulmonary pseudoaneurysm. B – displays a CT image revealing a new heterogeneously hyperdense structure in the superior left lower lobe measuring up to 1.9cm×2.9cm, which appears to demonstrate connection to a left lower lobe segmental pulmonary artery concerning for a pulmonary pseudoaneurysm. C – pulmonary angiography with embolization of superior left lower lobe segmental pulmonary artery with coil.
Pulmonary artery pseudoaneurysm (PAP) is a rare cause of hemoptysis, involving only the outer layer of the vessel wall, unlike true aneurysms which involve all three layers.1 The risk of rupture in PAPs is generally correlated with their size, with larger pseudoaneurysms carrying a higher risk.2 However, given the overall high rupture potential, prompt treatment is recommended regardless of size.1 Untreated PAPs pose a significant threat, as rupture can lead to massive hemoptysis with a high mortality rate.1,3
PAP typically presents with hemoptysis, though shortness of breath may also occur, either as a direct consequence of the PAP or secondary to hemoptysis.1 In some cases, however, PAP may be asymptomatic.1,3 Primary causes include infection, malignancy, and trauma, often iatrogenic.1 PAP has been documented as rare complications of various interventional procedures, including Swan-Ganz catheterization, right heart catheterization, biopsies, chest tube insertion3 and also mechanical thrombectomy.4 This case represents the first known occurrence following suction thrombectomy using the Inari Flowtriever system. The FLARE study5 evaluating the Flowtriever system for percutaneous mechanical thrombectomy reported a less than 4% incidence of major adverse events, including pulmonary vascular injury.
Prompt diagnosis via CT chest angiography in this case facilitated successful endovascular repair. Surgical options for PAP repair include pneumonectomy, lobectomy, pulmonary artery ligation, and direct arterial repair,3 but endovascular techniques such as transcatheter embolization offer a less invasive alternative with lower morbidity and mortality. Despite the risks associated with transcatheter embolization,3 the patient underwent successful coil embolization without complications.
This case highlights the clinical presentation and imaging findings of PAP, a rare condition, and underscores a novel complication following suction thrombectomy for pulmonary emboli. It emphasizes the importance of a multidisciplinary approach, involving diagnostic radiology, pulmonology, and interventional radiology, to ensure timely recognition and treatment of PAP, ultimately improving patient outcomes.
FundingNone.
Conflict of InterestNone for all authors.







