


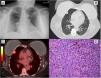
A 64-year-old active smoker with a history of breast cancer status postmastectomy presented with abnormal computed tomography (CT) of the chest for lung cancer screening. Physical examination was unremarkable. Chest radiography was unrevealed (Fig. 1A). CT of the chest revealed a 1.9cm×1.2cm subpleural right middle lobe(RML) lung nodule (Fig. 1B). F18-fluorodeoxyglucose positron emission tomography scan (Fig. 1C) showed intense uptake of RML nodule with no evidence aside from the tumor. The patient underwent lobectomy and pathology of the specimen (Fig. 1D) demonstrated rounded, nodules malignant cells and scattered areas of brown pigment deposition. Immunohistochemical stains, S100 is strongly and diffusely positive, consistent with pulmonary melanoma. To rule out the diagnosis of melanoma metastasis from a primary site, the patient underwent a thorough repeat skin examination which showed no dermatology lesion, and the patient denied any history of skin malignancy. These clinical and pathology features support the diagnosis of primary pulmonary melanoma (PPM). The patient was recovered well after surgery.
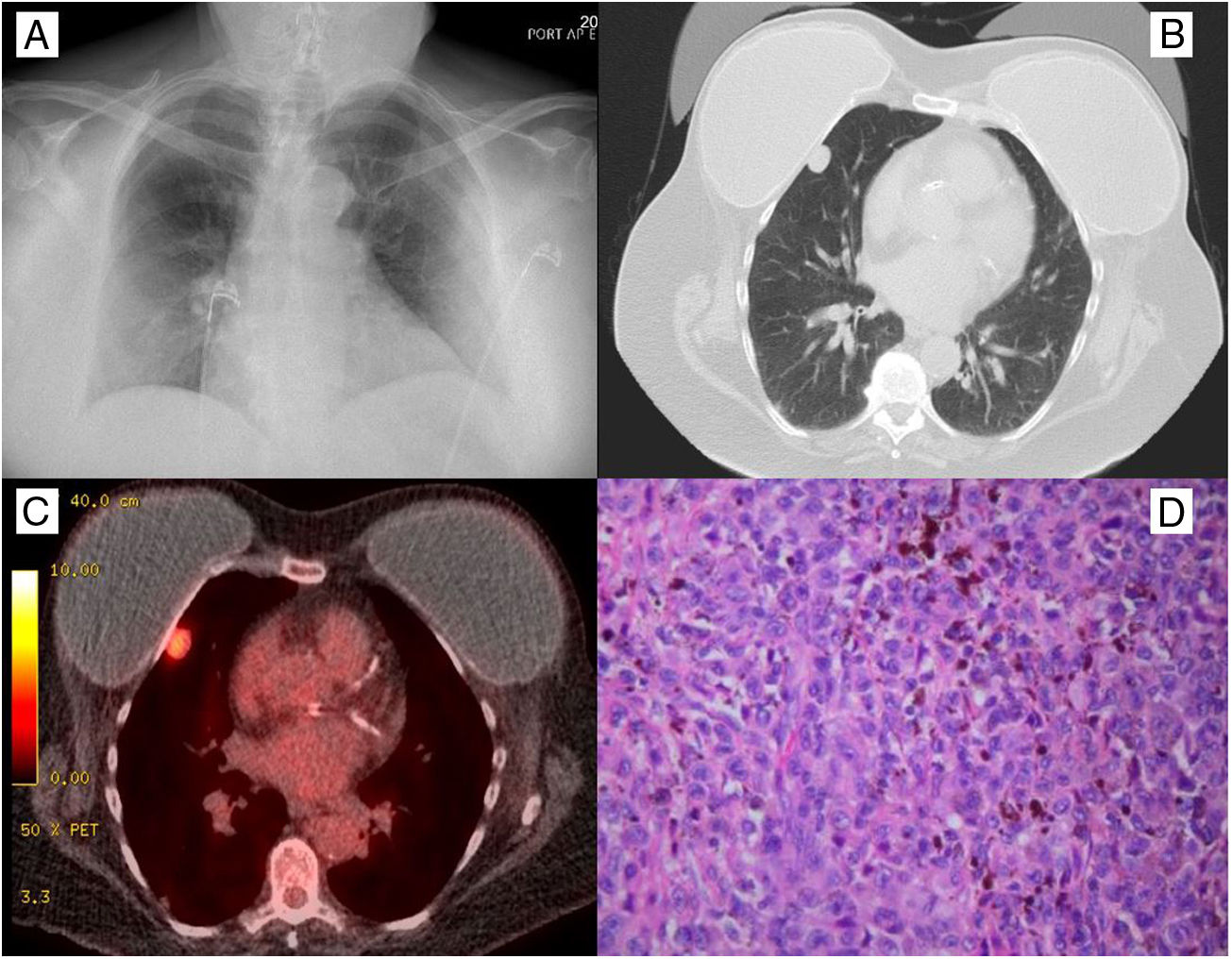
(A) Chest radiography was unremarkable. (B) Computed tomography of the chest demonstrated 1.9cm×1.2cm subpleural right middle lobe lung nodule. (C) F18-fluorodeoxyglucose positron emission tomography scan showed intense uptake in a nodule in the right middle lobe of the lung with no evidence of malignancy aside from the primary lung tumor. (D) Pathology of the resected specimen demonstrated the malignant cells form rounded nodules with thin fibrous rims. There are scattered areas with prominent coarse, brown pigment deposition. Cells are large with variable amounts of pink cytoplasm and form sheets. There are enlarged nuclei with irregular nuclear contours, vesicular chromatin, occasional multinucleation or nuclear inclusions, and some visible nucleoli consistent with melanoma.
PPM is found in only 0.01 percent of all lung tumors.1 The clinical manifestations of the disease were like the other thoracic malignancies, including cough, hemoptysis, dyspnea, chest pain, or incidental finding2 as in our case. A diagnosis is based on clinical and pathological criteria.3 The clinical criteria include an absence of either history of a previous melanoma or demonstrable melanoma outside the thorax at the time of surgery. The presence of a solitary lung tumor is required.3 The established pathological criteria incorporate immunohistochemical staining and evidence of melanoma cells or spindle cells arranged in fascicles.3 Lobectomy or pneumonectomy represents the best opportunity for long-term survival.1
FundingNone.
Conflict of InterestNone for all authors.







