

Lung cancer is the leading cause of cancer mortality worldwide, accounting for one in every five cancer-related deaths and responsible for approximately 18.7% of all cancer deaths in both sexes [1]. It is common to diagnose lung cancer at advanced stages, impacting its prognosis and survival [2]. The main risk factor associated with this type of cancer is tobacco smoking, however, occupational exposure to carcinogens and radon exposure are also well-known contributors to lung cancer burden. Of the 120 agents classified by the International Agency for Research on Cancer (IARC) as group 1 human carcinogens, 47 are of occupational origin [3]. Such exposures occur in a wide range of occupations, including mining, construction, glass and ceramic fiber work, and chemical manufacturing. Despite this, the evidence regarding occupational risk among women remains limited, since most studies have focused on men and subsequently extrapolated results to women [4–6]. Sex-specific results are therefore necessary.
Radon gas is recognized by the World Health Organization (WHO) as the second leading cause of lung cancer overall, and the leading cause among never-smokers [7]. Radon is a naturally occurring radioactive gas that can accumulate indoor, exposing the respiratory tract to ionizing radiation [8]. The WHO has recommended reference levels of 100Bq/m3[7]. While the interaction between radon and tobacco smoking has been well documented [9–12], evidence on the combined effect of radon, tobacco, and occupational exposures remains scarce [13].
The aim of this study was, first, to determine whether tobacco smoking modifies the effect of occupation on lung cancer risk, stratified by sex; and second, to analyze whether residential radon exposure modifies the effect of occupation on lung cancer risk, again stratified by sex.
We conducted a pooling study of five multicenter case-control studies carried out between 1992 and 2020 in hospitals located in Galicia, Castilla y León, Madrid, Asturias (Spain), and Oporto (Portugal). All original studies used comparable methodologies, allowing harmonization of variables and joint analysis in a single pooled database. Cases were histologically confirmed lung cancer patients, while hospital-based controls were frequency-matched by age and sex. Controls were patients admitted for conditions not related to lung cancer, such as orthopedic surgery, cataracts, lipomas, or inguinal hernias; as well as from uncomplicated microsurgical procedures, including carpal tunnel release or disk hernias. Only the controls from the first study [14] were selected from the 1991 Census, using stratified random sampling based on the sex distribution among cases and the population weighting of each sub-area.
Trained staff administered structured questionnaires to collect sociodemographic data, tobacco history, occupational history (up to five previous occupations and duration of each occupation), and residential information. Radon exposure was measured in dwellings using alpha-track devices over a minimum of three months, processed at the Galician Radon Laboratory. Of note, 788 participants lacked radon measurements, mainly because the detector was not returned by the participant. To minimize this issue, two follow-up phone calls were made to encourage return of the device. Occupations were coded according to ISCO-68, grouped at the major group level. Additionally, we created a category of “Housewives”.
We first performed logistic regressions stratified by sex, using “Administrative and managerial workers” and “Clerical workers” as reference groups, adjusting for age, smoking, and radon exposure. Odds ratios (ORs) and 95% confidence intervals (95%CIs) were estimated. To explore modification of effect, we fitted models with combined categories of occupation and smoking, and of occupation and radon, globally and by sex. Statistical significance was set at p<0.05, and analyses were performed in Stata v.17.
A total of 4203 participants (1987 cases and 2216 controls) were included, with 1288 women and 2915 men. Median age was higher among cases than controls in both sexes. The percentage of never smokers was higher among women (69.8% of female cases, 82.6% of female controls) compared with men (8.0% of male cases, 35.9% of male controls). For ever-smokers, cumulative tobacco consumption was similar in men and women, with cases being heavier smokers compared to controls. Residential radon exposure above 300Bq/m3 was slightly more frequent in cases than controls for both sexes. Cases and controls resided mainly in towns and countryside. Adenocarcinoma was the most frequent histologic type in women (63.7%), whereas squamous cell carcinoma predominated in men (29.2%).
In adjusted logistic regression models, several occupational categories were associated with increased lung cancer risk, with differences by sex. Among women, “Sales workers” (OR 5.19, 95%CI: 1.79–15.08), “Craft and related trades workers” (OR 1.96, 95%CI: 1.04–3.69), “Elementary occupations” (OR 5.12, 95%CI: 1.26–20.86), and “Housewives” (OR 2.61, 95%CI: 1.47–4.62) showed significant ORs. Among men, significant associations were observed for “Professional, technical and related workers” (OR 1.79, 95%CI: 1.10–2.90), “Service workers” (OR 1.65, 95%CI: 1.06–2.55), “Craft and related trades workers” (OR 1.70, 95%CI: 1.05–2.75), “Plant and machine operators” (OR 1.78, 95%CI: 1.19–2.65), and “Elementary occupations” (OR 1.69, 95%CI: 1.18–2.41).
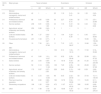
When analyzing the joint effect of tobacco smoking and occupation, we observed a possible modification effect among men. For instance, in men, “Professional, technical and related workers” showed ORs rising from 3.80 (95%CI: 1.01–14.27) among never-smokers to 22.89 (95%CI: 6.01–87.22) among smokers. Similarly, “Craft and related trades workers” presented an OR of 3.72 (95%CI: 1.03–13.40) among never-smokers, which increased to 37.54 (95%CI: 10.11–139.35) among smokers. Among women, this effect was less consistent, with some significant results such as “Service workers” (OR 3.44, 95%CI: 1.42–8.36) and “Housewives” (OR 16.66, 95%CI: 1.84–150.83) among smokers, but overall weaker trends (Table 1).
Tobacco use, major occupational groups (ISCO-68) and lung cancer risk, stratified by sex.
| ISCO-68 | Major groups | Never smokers | Exsmokers | Smokers | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | OR | 95%CI | n | OR | 95%CI | n | OR | 95%CI | ||
| Women | ||||||||||
| 2/3 | Administrative, managerial, clerical and related workers | 42 | 1 | – | 25 | 1.18 | 0.41–3.41 | 24 | 1.32 | 0.43–4.04 |
| 0/1 | Professional, technical and related workers | 88 | 0.85 | 0.38–1.89 | 30 | 2.27 | 0.84–6.14 | 32 | 7.75 | 2.51–23.86 |
| 5 | Service workers | 236 | 0.81 | 0.39–1.65 | 44 | 1.19 | 0.47–3.02 | 64 | 3.44 | 1.42–8.36 |
| 6 | Agricultural, animal husbandry and forestry workers | 250 | 0.86 | 0.42–1.79 | 3 | 1 | – | 3 | 1 | – |
| 7 | Craft and related trades workers | 98 | 1.37 | 0.62–3.01 | 11 | 1.44 | 0.32–6.39 | 4 | 5.45 | 0.51–58.60 |
| XI | Housewives/homemakers | 201 | 1.59 | 0.77–3.27 | 9 | 1 | – | 11 | 16.66 | 1.84–150.83 |
| XII | Other | 19 | 7.30 | 1.41–37.83 | 11 | 7.12 | 1.27–39.97 | 9 | 12.66 | 1.39–115.30 |
| Men | ||||||||||
| 2/3 | Administrative, managerial, clerical and related workers | 47 | 1 | – | 109 | 5.13 | 1.63–16.16 | 71 | 17.00 | 5.19–55.66 |
| 0/1 | Professional, technical and related workers | 41 | 3.80 | 1.01–14.27 | 101 | 9.32 | 2.95–29.48 | 32 | 22.89 | 6.01–87.22 |
| 4 | Sales workers | 23 | 3.55 | 0.84–14.95 | 41 | 18.18 | 4.93–67.04 | 26 | 51.20 | 10.72–244.48 |
| 5 | Service workers | 59 | 3.14 | 0.90–11.00 | 129 | 7.29 | 2.35–22.64 | 93 | 29.28 | 8.81–97.38 |
| 6 | Agricultural, animal husbandry and forestry workers | 175 | 0.87 | 0.27–2.83 | 228 | 6.49 | 2.15–19.63 | 140 | 8.29 | 2.69–25.52 |
| 7 | Craft and related trades workers | 41 | 3.72 | 1.03–13.40 | 96 | 6.45 | 2.02–20.59 | 59 | 37.54 | 10.11–139.35 |
| 8 | Plant and machine operators | 99 | 2.80 | 0.86–9.07 | 186 | 10.76 | 3.54–32.66 | 111 | 19.25 | 6.11–60.68 |
| 9 | Elementary occupations | 166 | 1.26 | 0.39–4.07 | 472 | 11.97 | 4.07–35.22 | 309 | 19.95 | 6.68–59.59 |
| XII | Other | 10 | 7.48 | 1.18–47.34 | 30 | 18.48 | 4.30–79.45 | 13 | 47.87 | 8.30–276.01 |
Results shown for groups having more than 30 participants in at least one stratum.
Regarding radon exposure, effect modification by occupation was suggested for both sexes, however, results at lower exposure levels were not statistically significant. Among women exposed to >300Bq/m3, risks were particularly high for “Craft and related trades workers” (OR 5.77, 95%CI: 1.42–23.37) and “Housewives” (OR 3.58, 95%CI: 1.14–11.21). Among men in the same exposure category, “Craft and related trades workers” showed an OR of 5.80 (95%CI: 1.46–23.05) (Table 2).
Residential radon, major occupational groups (ISCO-68) and lung cancer risk, stratified by sex.
| ISCO-68 | Major groups | <100Bq/m3 | 100–300Bq/m3 | >300Bq/m3 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Women | n | OR | 95%CI | n | OR | 95%CI | n | OR | 95%CI | |
| 2/3 | Administrative, managerial, clerical and related workers | 28 | 1 | – | 39 | 1.22 | 0.43–3.43 | 17 | 0.26 | 0.06–1.17 |
| 0/1 | Professional, technical and related workers | 44 | 2.34 | 0.85–6.45 | 70 | 1.24 | 0.48–3.16 | 25 | 0.75 | 0.22–2.53 |
| 5 | Service workers | 23 | 0.98 | 0.39–2.46 | 149 | 0.99 | 0.41–2.39 | 52 | 1.30 | 0.49–3.47 |
| 6 | Agricultural, animal husbandry and forestry workers | 55 | 0.93 | 0.34–2.52 | 109 | 1.04 | 0.42–2.62 | 41 | 2.24 | 0.78–6.39 |
| 7 | Craft and related trades workers | 18 | 0.96 | 0.27–3.40 | 62 | 1.51 | 0.58–3.93 | 18 | 5.77 | 1.42–23.37 |
| XI | Housewives/homemakers | 81 | 1.87 | 0.74–4.74 | 84 | 2.29 | 0.90–5.80 | 32 | 3.58 | 1.14–11.21 |
| Men | n | OR | 95%CI | n | OR | 95%CI | n | OR | 95%CI | |
|---|---|---|---|---|---|---|---|---|---|---|
| 2/3 | Administrative, managerial, clerical and related workers | 73 | 1 | – | 90 | 0.68 | 0.34–1.37 | 29 | 1.19 | 0.45–3.13 |
| 0/1 | Professional, technical and related workers | 52 | 1.85 | 0.83–4.10 | 67 | 1.59 | 0.75–3.37 | 27 | 0.87 | 0.31–2.47 |
| 4 | Sales workers | 37 | 1.09 | 0.45–2.65 | 27 | 7.76 | 2.49–24.24 | 7 | 5.58 | 0.76–41.12 |
| 5 | Service workers | 99 | 1.47 | 0.74–2.90 | 75 | 1.49 | 0.72–3.09 | 39 | 0.84 | 0.35–2.01 |
| 6 | Agricultural, animal husbandry and forestry workers | 273 | 0.43 | 0.23–0.78 | 115 | 1.24 | 0.64–2.43 | 40 | 0.99 | 0.41–2.36 |
| 7 | Craft and related trades workers | 69 | 0.93 | 0.44–1.95 | 65 | 1.55 | 0.73–3.31 | 17 | 5.80 | 1.46–23.05 |
| 8 | Plant and machine operators | 138 | 1.09 | 0.57–2.08 | 126 | 1.93 | 1.00–3.70 | 57 | 1.61 | 0.74–3.52 |
| 9 | Elementary occupations | 371 | 1.04 | 0.59–1.83 | 270 | 1.72 | 0.96–3.10 | 112 | 1.77 | 0.91–3.46 |
Results shown for groups having more than 30 participants in at least one stratum.
Our findings suggest that both tobacco smoking and residential radon exposure may modify the effect of occupational exposures on lung cancer risk, particularly among men. To our knowledge, this is the first study to assess potential modification between occupation and radon exposure in a general population. Previous research on miners has described submultiplicative interactions between radon and smoking [15,16], whereas our data indicate that residential radon could have an independent and possibly additive effect in the general population.
Sex differences observed in this study may reflect not only biological factors, such as hormonal influences and endocrine interactions with tobacco [17,18], but also differences in occupational distribution between men and women. Men predominate in heavy industrial trades, while women are more frequently represented in service jobs, where exposures may differ. These results align with previous reports, highlighting the importance of considering sex in occupational cancer epidemiology [4,5].
The main limitation of this work lies in the use of ISCO-68 major groups, which pool heterogeneous occupations within broad categories. This may mask risks specific to certain jobs or industries. Additionally, our analysis was based on occupational categories rather than direct assessment of occupational exposures. A more descriptive analysis linking specific exposures with lung cancer risk would provide additional results. Interaction models were not conducted due to sample size limitations, so we opted for stratified analyses as an exploratory approach. Future studies with larger sample sizes will be needed to evaluate interaction terms with greater statistical power. Finally, stratification by sex, radon, and smoking inevitably reduced sample sizes in some subgroups, limiting statistical power. Strengths of this study include its large sample size, adjustment for residential radon exposure (not usually considered in previous studies) and sex-stratified analyses.
In conclusion, our study indicates that occupational risk of lung cancer may be modified by tobacco smoking and, to a lesser extent, by residential radon exposure. These effects differ by sex, with stronger associations observed among men. Our results highlight the need for preventive strategies such as smoking cessation programs directed to workers exposed to occupational carcinogens, radon mitigation in radon-prone areas and the consideration of occupational history into lung cancer screening.
Author contributionEliana Torres-Cadavid: conceptualization, resources, data curation, writing – original draft. Cristina Candal-Pedreira: conceptualization, methodology, formal analysis, investigation, writing – review & editing. Alberto Ruano-Ravina: Conceptualization, methodology, data curation, supervision, writing – review & editing. Karl Kelsey: writing – review & editing. Lucía Martín-Gisbert: investigation, writing – review & editing.
Ethics approvalThe original studies protocols, funding and informed consent models were approved by the relevant Clinical Research Ethics Committees.
DeclarationThis scientific letter forms part of the work leading to the doctoral thesis of Eliana Torres Cadavid.
Artificial intelligence involvementNo artificial intelligence tools were used in process of this study. All work was carried out by the authors.
FundingNo funding was received.
Conflicts of interestDr. Kelsey is a founder and scientific advisor to Cellintec which had no role in this research. The remaining authors declare there are no conflicts of interest that are relevant to the publication of this paper.
The followings are the supplementary data to this article:








