

Asthma management should address both current control and future risk [1], with prevention of exacerbations being a key therapeutic objective. Exacerbations impose a substantial clinical and healthcare resource burden [2]. Numerous risk factors for asthma exacerbations have been described and can be broadly grouped into demographic, environmental exposures, comorbidities and treatment related factors. Biomarkers for asthma exacerbations such as low forced expiratory volume in the first second (FEV1), bronchodilator reversibility, elevated serum and sputum eosinophils, and increased fractional exhaled nitric oxide (FeNO) have been proposed [2,3]. Patients with such risk factors may require closer monitoring to prevent treatment failure [4].
Asthma is characterized by chronic airway inflammation and oxidative stress, leading to peroxidation of membrane lipids and the subsequent generation of volatile organic compounds (VOCs) detectable in exhaled breath [5,6]. These VOCs act as metabolic fingerprints of airway biochemical activity and have been proposed as noninvasive markers of inflammatory processes. Among them, propanoic and nonanoic acids have received increasing attention [7]. Nonanoic acid reflects oxidation of aldehydes under high oxidative conditions, whereas propanoic acid—a short-chain fatty acid—can arise both from lipid peroxidation and from airway microbial metabolism [5]. Prior studies have explored VOCs for diagnostic purposes, particularly in populations where conventional tools perform poorly, such as smokers [7]. While specific VOC signatures have been associated with inflammatory phenotype [6], their potential utility for predicting asthma exacerbation risk remains unclear.
We hypothesized that asthma patients with clinical risk factors for exacerbations would display a distinct exhaled VOC pattern, particularly involving lipid peroxidation-derived acids, which could help guide personalized monitoring and treatment strategies.
A multicenter, cross-sectional study was conducted across five specialized asthma units in Madrid (Spain). Adult patients with confirmed asthma diagnosis and good adherence to maintenance therapy were consecutively recruited. This protocol was approved by local Ethics Committees, and all participants provided written informed consent.
Patients with other pulmonary diseases, recent exacerbations or infections (<1 month), or recent use of systemic corticosteroid or biologic therapy, active or previous malignancy, ischemic heart disease, or relevant endocrine disorders were excluded. Comorbidities were systematically recorded and managed according to current recommendations. Asthma diagnosis, control level, and severity were assessed according to the Spanish Guidelines for the Management of Asthma (GEMA) [1]. Severe exacerbations in the previous year (requiring systemic corticosteroids ≥3 days) were recorded. Patients were classified as being at risk of exacerbation if they fulfilled any risk criteria [3]: uncontrolled asthma, obesity, active smoking, persistent airway obstruction (FEV1<60% predicted), or high type 2 inflammation (FeNO>40ppb or serum eosinophils>300cells/μL).
To minimize potential sources of variability, all exhaled breath samples were collected between 9 and 11am to avoid the potential influence of diurnal fluctuations. Participants were instructed to abstain from smoking, eating, or drinking for at least one hour prior to sampling to avoid contamination. Three consecutive forced expirations were combined into one pooled Bio-VOC® (Markes International, UK) breath samplers. Ambient air was simultaneously sampled to exclude environmental interference. VOCs were trapped on thermal desorption tubes and analyzed within 24h by thermal desorption–gas chromatography–mass spectrometry (TD–GC–MS). Calibration was repeated after any modification or replacement of components in the TD–GC–MS system, and identification was achieved by comparison with the NIST library. A qualitative approach was used. The analyzed VOCs were hexanal, heptanal, nonanal, propanoic acid, and nonanoic acid, previously validated by our group [5,8]. Only compounds with an exhaled-to-ambient air ratio>1 were considered endogenous and included in the analyses [5]. The analytical method followed ICH Q2(R2) validation standards [9]. All analyses were performed by a blinded operator.
Multivariate approaches (e.g., PCA-based clustering and supervised classifiers such as PLS-DA) were initially considered, but were discarded due to the small number of VOCs and limited dimensionality. Because only five VOCs were analyzed and each showed distinct biochemical relevance, we conducted compound-by-compound analyses. Descriptive and inferential statistics were performed using Stata®. Regression models were fitted using a prespecified strategy based on established exacerbation-risk factors to reduce confounders and to explore associations between VOCs and clinical variables. A Bonferroni correction for multiple comparisons was applied. Statistical significance was set at p-value<0.05. No data-driven variable selection was applied in order to avoid model overfitting. The sample size was justified based on the requirements for stable multivariable logistic regression. Assuming a minimum of 10 outcome events per predictor variable, and anticipating inclusion of up to 8 covariates in the adjusted models, at least 80 events were required. Based on previous asthma cohorts with similar characteristics, we expected approximately 40–50% of patients to meet exacerbation-risk criteria, requiring a total sample size of approximately 100–120 participants.
A total of 120 patients were included. Mean age was 64.3 years (SD 18.9); 71.7% female; mean body mass index 27.1kg/m2 (SD 4.7). 48.3% were never smokers, and mean asthma control test (ACT) score was 22.7 (SD 3.2). Mean FEV1 was 95.5% of the predicted value (SD 18.7), FeNO 30ppb (SD 33.8), and blood eosinophils 281cells/μL (SD 224). 48.3% were non-allergen sensitized, and 35.0% had chronic rhinosinusitis. According to GEMA control criteria [1], 17 patients (14.2%) were poorly controlled, 69 (57.5%) were partially controlled, and 34 (28.3%) were well controlled. The presence of VOCs showed no significant association with asthma control status [1] (Supplementary material, Table 1).
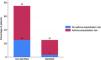
When VOC profiles were analyzed according to Global Initiative for Asthma (GINA)-defined exacerbation risk [3], only propanoic acid showed a significant association with exacerbation risk factors (odds ratio (OR) of 3.25; 95% CI 1.04–10.15; p=0.027) (Fig. 1). Propanoic acid was present in 25% (30 patients), with a higher frequency among those at risk of exacerbations (86.7%) (Fig. 2). In the multivariate logistic regression model adjusting for tobacco exposure, sex, FEV1, FeNO, blood eosinophil counts, age, asthma severity and the number of severe exacerbations in the previous year as covariates, only the number of severe exacerbations remained associated with the presence of exhaled propanoic acid (OR=1.82; 95% CI, 1.06–2.13; p=0.031) (Supplementary material, Table 2). However, the overall model did not reach statistical significance (p=0.17), likely due to interindividual variability or limited statistical power. Although propanoic acid was more frequently detected in patients with a history of exacerbations, no significant linear trend was observed when VOCs were analyzed according to the number of exacerbations during the past year (Supplementary material, Table 4).


A positive bronchodilator response (increase in FEV1 of at least 12% and 200mL from baseline) during follow-up was observed in 12 patients (10%), with no significant differences between asthma control groups (Supplementary material, Table 2).
In this multicenter study, propanoic acid was detected more frequently in the exhaled breath of asthma patients presenting clinical risk factors for exacerbations. Due to the characteristics of the study, this association should be interpreted as exploratory and requires confirmation in longitudinal studies.
Compared with previous VOC studies, our work provides insight into real-world exacerbation risk factors rather than focusing solely on inflammatory phenotypes. Analysis of exhaled VOCs reflects airway biochemical activity and has been proposed as a noninvasive complementary tool for asthma assessment [10]. The field of breathomics must transition from the academic research setting to clinical implementation through standardization of the technique and reproducibility in real-world conditions, adjusting for confounders.
Propanoic acid has been investigated in asthma for diagnostic and mechanistic purposes. From a biological standpoint, the association between elevated exhaled propanoic acid and exacerbation risk may reflect a complex interplay between airway inflammation, oxidative stress, and microbial activity. Compared with established exacerbation-risk indicators, propanoic acid may capture an additional oxidative-stress-related signal not reflected by traditional biomarkers. This stress could promote persistent subclinical inflammation and epithelial vulnerability, which may ultimately predispose patients to future exacerbations, supporting its potential utility as an early biomarker of exacerbation-prone asthma.
This study has limitations that should be taken into account. First, this study is exploratory in nature, and the findings should be interpreted as hypothesis-generating rather than confirmatory. The cross-sectional design does not allow evaluation of temporal relationships, and therefore the potential role of propanoic acid as a biomarker of future exacerbations remains speculative. Although propanoic acid showed an association in univariate analyses, the overall multivariable model did not reach statistical significance, suggesting that the observed relationships may be influenced by interindividual variability and limited statistical power. Strengths of the study include its multicenter design, standardized sampling and analysis procedures, and the inclusion of a well-characterized population. These features enhance the reliability of the results and support the potential clinical applicability of exhaled VOC profiling.
In conclusion, propanoic acid was more frequently detected in the exhaled breath of patients with clinical risk factors for exacerbations. However, these preliminary results should be interpreted as hypothesis-generating. Longitudinal validation studies with quantitative VOC assessment are needed to clarify the biological significance and potential clinical utility of propanoic acid in identifying patients at increased risk of future exacerbations.
Author contributorsRMDC and CMM contributed substantially to the study design, data acquisition, and interpretation of the results. MJG contributed to interpretation of the results and contributed to the drafting and critical revision of the manuscript. CCS, ATA, ALV, RGG, IB, JJJE, MAML were involved in data acquisition and contributed to the drafting and critical revision of the manuscript. All authors reviewed and approved the final version of the manuscript.
Ethical approvalThis study was approved by the Medical Research Ethics Committee.
Artificial intelligenceArtificial intelligence tools were used in the preparation of this manuscript for grammar correction and language refinement. All content was subsequently reviewed and validated by the authors to ensure accuracy and scientific integrity.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interestThe authors declare no conflicts of interest related to the content of this publication.
This project was endorsed by the Research Committee of the Spanish Society of Pulmonology and Thoracic Surgery (SEPAR).
The followings are the supplementary data to this article:








