





Day Hospital units specialized in pulmonology are a relatively new instrument for providing care to complex respiratory patients. However, the number of studies focused on the efficacy and efficiency of Day Hospitals is scarce.
AimTherefore, the aim of the present study was to analyze the effects of implementing a specialized respiratory Day Hospital in a standard teaching hospital with 500 beds.
MethodsAn analysis of efficacy, efficiency, and quality care.
ResultsThroughout the study period (2 years) the Day Hospital progressively increased its activity. Although patient pressure on the emergency department remained constant, this was associated with a parallel increase in the overall medical activity of the hospital. However, there was a reduction in the number of admissions, and consequently in the need for beds in the Pulmonology Department. The complexity of the hospitalized patients increased, although the efficiency (standard functioning ratio) and quality (readmissions and mortality) of patient care remained stable.
ConclusionDay Hospital pulmonology units are a useful tool in the management of respiratory patient care. They reduce the need for hospitalizations, while maintaining healthcare quality and complementing other care management instruments.
Los hospitales de día de neumología constituyen un instrumento relativamente nuevo de atención al paciente respiratorio complejo. Faltan estudios sobre su eficacia y eficiencia.
ObjetivoEstudiar el impacto de la instauración de un hospital de día neumológico en una institución terciaria de 500 camas.
MetodologíaAnálisis de eficacia, eficiencia y calidad.
ResultadosEn el período analizado (2 años) el hospital de día incrementó progresivamente su actividad. Esto se acompañó de mayor actividad clínica global en neumología, pero también de una reducción en el número de altas hospitalarias, aunque en el período estudiado no varió la presión de pacientes sobre urgencias. Como consecuencia, también se redujo la necesidad de camas en la sala de hospitalización convencional. Por otra parte, aumentó la complejidad de los pacientes ingresados, aunque la eficiencia (razón de funcionamiento estándar) y calidad (reingresos y mortalidad) de la atención en ese dispositivo se mantuvieron estables.
ConclusionesLos hospitales de día neumológicos constituyen un instrumento útil en la gestión de la atención a pacientes respiratorios, ya que reducen las necesidades de hospitalización, manteniendo la calidad asistencial y complementando otros dispositivos.
The consumption of resources by the patient suffering from a respiratory condition is very high, as it is one of the main causes of the request for hospitalization.1,2 This typically involves a certain imperativeness in terms of response, which varies depending on the season of the year. Especially during the winter months, the pressure on care-providers can lead to problems in the management of the resources assigned to patients.3 Traditionally, the activity generated by patients with respiratory problems has centred around casualty and conventional hospital wards. In recent years, however, other forms of medical attention have been added to the system. Prominent among them are the Day Hospitals4–6 and the short stay units,7 both within the general structure, and specifically dependent on the Pneumonology Services. The idea underlying the appearance of these new ways of managing the demand for attention on the part of those suffering from respiratory conditions is to improve and streamline the allocation of resources.8 This is achieved by means of a careful selection of patients, and an appropriate and targeted treatment for each type and phase of the illness.7,8
Day Hospitals imply an important change in the way in which the problems associated with respiratory illness are approached, as they enable the level of diagnostic and therapeutic intensity to be maintained without the huge costs normally entailed by hospitalization (approximately 420€ per day as opposed to 270€ per day in a Day Hospital). Candidates for both types of hospital are often elderly patients with serious co-morbidities, though they differ as regards the level of risk and the treatment and supervision requirements. It is precisely to these subjects, as they do not benefit at all from being confined to hospital (de-conditioning, additional infections) and do not like to be far removed from their familiar environment, that the Day Hospital is best suited, providing that their condition permits it. The first experiments in this type of hospital were for psychiatric patients, those who had received surgery and those with onco-hematological malignancy,10–12 and it has proven extremely useful in dealing with the associated pathologies.13 With the passing of time, different Day Hospital models have developed, both in general practice and specialized orientation. The latter make it possible to offer a range of diagnostic and therapeutic approaches with more specific profiles, and greater complexity in the techniques employed. Despite this, there are few studies that systematically evaluate the impact of Pulmonology Day Hospitals in the management and efficiency of the services that they depend on. The aim of the present study was to analyse the consequences of the implementation of a Day Hospital specializing in respiratory illnesses on the consumption of resources, the efficiency and the quality of hospital attention.
Material and MethodsThis is a retrospective study on the health care activity at the Pulmonology Service of a public university hospital, carried out during 2007 and 2008. When relevant, the previous year was also studied. The centre, with 500 beds for patients with acute treatments, caters for a population of approximately 316,000 inhabitants, in an area with a strong social demand and considerable access to hospital services (96/1000). The organizational structure of the Pulmonology Service can be seen in Fig. 1, and it must be pointed out that the centre also has a Thoracic Surgery Service.

The Hospital de Día Neumológico (Pulmonology Day Hospital) was started at the end of 2006, one year after the Unidad Neumológica de Estancia Corta7 (Pulmonology Short Stay Unit), and two years after the Reforma de la Atención Specializada (RAE) (Specialised Care Reform) for the area in question. However, its definitive establishment coincided with the specific period of the present study (2007–2008).
All the data were collected by means of the centre's own digital system for the processing of health-care related information, which record the details concerning all the patient's visits to casualty, their external consultations, their conventional hospitalization, and their contacts with short-stay units and Day Hospitals. The analysis of the data was carried out at two levels:
- 1.
Information concerning the general activity of the Pulmonology Service, with a view to determining the evolution of the patients attended to in each case, as well as the impact of the Day Hospital on the number of patients attended to or hospitalized, and on the demand for complementary examinations, among other variables. In order to best determine the tendencies during the period in question, the decision was made to analyse the data by three-month periods.
- 2.
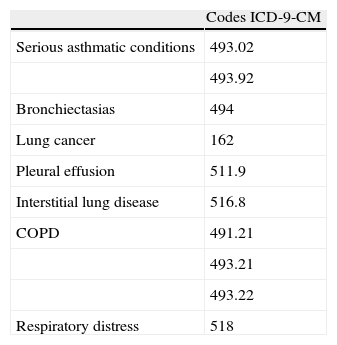
Simultaneously, (subanalysis) the subgroup of patients was analysed whose diagnosis would make them eligible for admission for treatment to the Day Hospital (Table 1). The criteria for such admission correspond to those established in the International Classification of Diseases (9th revision, clinical modification) (ICD-9-CM). The means whereby these patients were identified was the Basic Minimum Data Set analysis for the period under investigation, with the main focus being on the above mentioned diagnoses. Once the patient had been identified, information was sought concerning his or her contacts with the system during this period: that is to say, every institutional activity register in which the patient's name appeared. In order to obtain a better understanding of the data of the study, this section also includes data corresponding to the previous year (2006), when the first phase of the scheme was implemented.
Table 1.Pathologies Defined as Eligible for Attention in the Day Hospital.
Codes ICD-9-CM Serious asthmatic conditions 493.02 493.92 Bronchiectasias 494 Lung cancer 162 Pleural effusion 511.9 Interstitial lung disease 516.8 COPD 491.21 493.21 493.22 Respiratory distress 518 Abbreviations: IDC-9-CM, International Classification of Diseases, 9th revision, Clinical Modification; COPD, chronic obstructive pulmonary disease.
The normality of the variables was evaluated by means of the Kolmogorov–Smirnov test, and the QQ plot method, represented in the form of mean and standard deviation (x±S.D), or as total percentages. In order to analyse the three-monthly evolution of the variables, the adjusted trend line obtained by linear regression was used. For the comparison among the different years the method used was the χ2 test, or the variance analysis for repeated measurements, depending on the characteristics of the variable. The level of significance was established at P<.05.
ResultsAnalysis of the General Activity in Respiratory IllnessesDuring the period in question, a total of 155,985 emergencies were dealt with in the hospital. Of them, 2.78% were of a medical nature, and the others were surgical, gynecological, pediatric or patients in a critical condition. During the same period there were 161,253 hospital admissions, 40% of which were of a medical nature. On the other hand, respiratory conditions accounted for a little more than a quarter of all the medical activity carried out in the medical area, and with adult patients. (2526 out of a total of 9056 admissions), with a degree of complexity that was significantly superior to that of other pathologies [weight of Diagnosis Related Groups (DRG) being 1.945 as opposed to 1.7707 in the medical area as a whole]. The number of respiratory patients attended to and the complexity of their conditions were greater than those of other medical specialisms, such as the digestive apparatus or the cardio-circulatory system (1398 patients and a specific weight of 1.7064; and 1446 patients with a specific weight of 1.5797, respectively). On the other hand, the respiratory pathology that gave rise to most admissions was Chronic Obstructive Pulmonary Disease (COPD) (34%) followed by pneumonias (21%), other pulmonary infections (8%), asthma and pulmonary neoplasis (6% in each case). All these figures refer to the hospital as a whole as, although patients with respiratory disorders are treated mainly in pulmonology, they are also dealt with in other specialist areas like internal medicine or geriatrics.
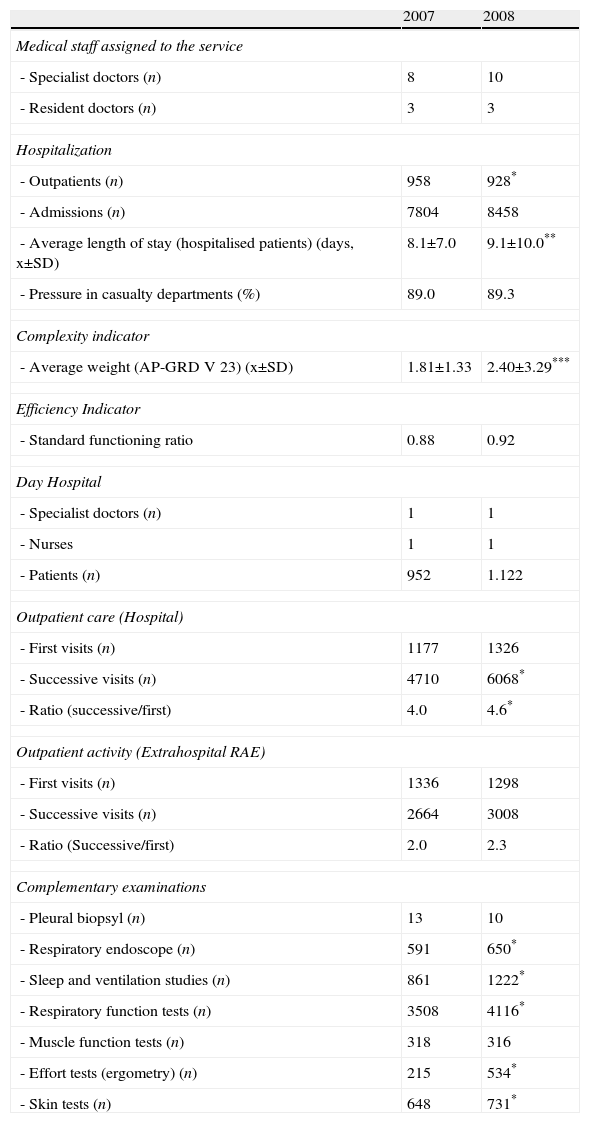
Centering our attention on the Pulmonology Service, and despite continued pressure in casualty during the period of our study, hospital admissions fell slightly during this same period (Table 2). This reduction was parallel to a significant increase in the complexity of the attention required (33%) (Fig. 2 and Table 2). Average length of stay in the Pulmonology Service also increased (12%) (Fig. 3 and Table 2), albeit with considerable variation between three-month periods. Nevertheless, however, appropriate efficiency was maintained if the average period of hospitalization was adjusted in accordance with the mix of pathologies (standard working ratio or SWR,14 0.88 for 2007 and 0.92 for 2008). This indicates that the increases in complexity were absorbed by a more efficient management of the patients. Furthermore, the reduced need for conventional hospitals led to a reduction in the number of beds theoretically assigned to this system (Table 3).
Indicators of Resources and General Activity in the Pulmonology Service.
| 2007 | 2008 | |
| Medical staff assigned to the service | ||
| - Specialist doctors (n) | 8 | 10 |
| - Resident doctors (n) | 3 | 3 |
| Hospitalization | ||
| - Outpatients (n) | 958 | 928* |
| - Admissions (n) | 7804 | 8458 |
| - Average length of stay (hospitalised patients) (days, x±SD) | 8.1±7.0 | 9.1±10.0** |
| - Pressure in casualty departments (%) | 89.0 | 89.3 |
| Complexity indicator | ||
| - Average weight (AP-GRD V 23) (x±SD) | 1.81±1.33 | 2.40±3.29*** |
| Efficiency Indicator | ||
| - Standard functioning ratio | 0.88 | 0.92 |
| Day Hospital | ||
| - Specialist doctors (n) | 1 | 1 |
| - Nurses | 1 | 1 |
| - Patients (n) | 952 | 1.122 |
| Outpatient care (Hospital) | ||
| - First visits (n) | 1177 | 1326 |
| - Successive visits (n) | 4710 | 6068* |
| - Ratio (successive/first) | 4.0 | 4.6* |
| Outpatient activity (Extrahospital RAE) | ||
| - First visits (n) | 1336 | 1298 |
| - Successive visits (n) | 2664 | 3008 |
| - Ratio (Successive/first) | 2.0 | 2.3 |
| Complementary examinations | ||
| - Pleural biopsyl (n) | 13 | 10 |
| - Respiratory endoscope (n) | 591 | 650* |
| - Sleep and ventilation studies (n) | 861 | 1222* |
| - Respiratory function tests (n) | 3508 | 4116* |
| - Muscle function tests (n) | 318 | 316 |
| - Effort tests (ergometry) (n) | 215 | 534* |
| - Skin tests (n) | 648 | 731* |
Abbreviations: AP-GRD V 23, Diagnostic Related Groups for all patients in version 23; RAE, Reforma de la Asistencia Especializada (Specialised Care Reform) (extra-hospital); X, media; SD, Standard Deviation. Changes between 2007 and 2008: *P<.05; **P<.01; ***P<.001. Admissions and patients, calculation across the entire area. Vis its and examinations, calculation based on the concept total for each case.
 and their complextity (thin line) during the period of the study.The tendencies appear as broken lines.")
. The tendency appears as a broken line.")
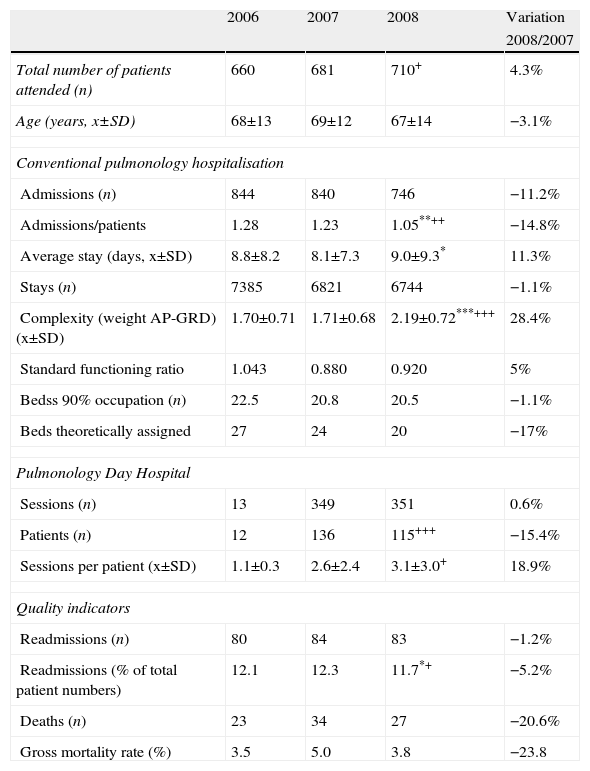
Activity Indicators in the Sub-analysis of Patients Whose Diagnosis Makes them Eligible for Admission to the Day Hospital (Data for the Day Hospital and for Conventional Hospitalization).
| 2006 | 2007 | 2008 | Variation | |
| 2008/2007 | ||||
| Total number of patients attended (n) | 660 | 681 | 710+ | 4.3% |
| Age (years, x±SD) | 68±13 | 69±12 | 67±14 | −3.1% |
| Conventional pulmonology hospitalisation | ||||
| Admissions (n) | 844 | 840 | 746 | −11.2% |
| Admissions/patients | 1.28 | 1.23 | 1.05**++ | −14.8% |
| Average stay (days, x±SD) | 8.8±8.2 | 8.1±7.3 | 9.0±9.3* | 11.3% |
| Stays (n) | 7385 | 6821 | 6744 | −1.1% |
| Complexity (weight AP-GRD) (x±SD) | 1.70±0.71 | 1.71±0.68 | 2.19±0.72***+++ | 28.4% |
| Standard functioning ratio | 1.043 | 0.880 | 0.920 | 5% |
| Bedss 90% occupation (n) | 22.5 | 20.8 | 20.5 | −1.1% |
| Beds theoretically assigned | 27 | 24 | 20 | −17% |
| Pulmonology Day Hospital | ||||
| Sessions (n) | 13 | 349 | 351 | 0.6% |
| Patients (n) | 12 | 136 | 115+++ | −15.4% |
| Sessions per patient (x±SD) | 1.1±0.3 | 2.6±2.4 | 3.1±3.0+ | 18.9% |
| Quality indicators | ||||
| Readmissions (n) | 80 | 84 | 83 | −1.2% |
| Readmissions (% of total patient numbers) | 12.1 | 12.3 | 11.7*+ | −5.2% |
| Deaths (n) | 23 | 34 | 27 | −20.6% |
| Gross mortality rate (%) | 3.5 | 5.0 | 3.8 | −23.8 |
Abbreviations: AP-DRG V23, Diagnosis related groups for all patients, version 23; X, mean; SD, Standard Deviation. Changes between 2007 and 2008: *P<.05; **P<.01; ***P<.001. Changes between 2006 and 2008: +P<.05; ++P<.01; +++P<.001.
The pulmonology Service attended to an average of 700 patients per three-month period, with a slight upward trend (Fig. 4a). During the same period, the Day Hospital showed a sustained increase in its activity, which was compensated for by the reduction in activity in other care areas in the same service (Fig. 4b). To be precise, and despite a certain oscillation, the number of patients attended to in the Pulmonology Day Hospital increased from 170 in the first three-month period of 2007 to 320 at the end of 2008. With regard to relative activity, that of the Day Hospital increased from 27% to 45% during this period, while there was a spectacular drop in pulmonological attention in casualty and in conventional hospital admissions. It is interesting to note that most of the care provided in the Day Hospitals is programmed on the same day, which suggests that they require rapid response treatment and are automatically channeled towards the new system. In fact, the percentage of this kind of visit rose from 35% at the beginning to 60% at the end of the period (Fig. 5).
. (a) The total number of patients is reflected as a continuous line, while the tendency is reflected as a broken line. (b) Detailed information corresponding to each of the systems for attending to patients (Day Hospital, Specialised Casualty Departments and Conventional Hospitalisation), in absolute values.")
Graphic representation of the three-monthly variation for patients attended by the Pulmonology Service in the different systems available (not counting scheduled external consultations). (a) The total number of patients is reflected as a continuous line, while the tendency is reflected as a broken line. (b) Detailed information corresponding to each of the systems for attending to patients (Day Hospital, Specialised Casualty Departments and Conventional Hospitalisation), in absolute values.
 and percentage of visits scheduled and dealt with on the same day (thin line). The tendencies are represented as broken lines.")
As it has already been mentioned, for this sub-analysis those patients were selected with a condition that could be seen to in the Day Hospital (pre hoc criteria, Table 1), and a comparative analysis was carried out with conventional hospital admissions activity (Table 3). The complementary data from the period of implementation of the new system (end of 2006) also appear in Table 3.
During the period of the study, the total number of patients attended to for the reasons specified across all the pulmonology treatment systems increased, while hospital admissions tended to decrease. The so-called admissions ratio (hospital admissions per patient attended to), also decreased steadily (Table 3). In the case of the patients in this subgroup, the average weighting increased by 28%, and although the average length of the stay also increased, the effectiveness (expressed as RFE) was somewhat greater. The accumulated reduction in the occupation of hospital beds, as a result of the activity of the Pulmonology Day Hospital, was 17% during the period in question. On the other hand, the number of sessions per patient in this system increased steadily, and reached 3.1±3.0 in 2008.
46% of the patients were direct access (patients already treated in the Day Hospital), 31% were directed to the service by the pulmonologist on duty, and 18% by other members of the service (external consultation and RAE 16%). It is worth pointing out that the general casualty service must notify the pulmonologist on duty before a patient is admitted to the Day Hospital, for which reason the latter mode of admission was exceptional. The specific complexity (AP-GRD) of the patients attended to in the Day Hospital was 1.76±0.65, with a Charlson co-morbidity index of 1.9±0.2. On the other hand, the procedures employed most frequently were vigilance and supervision of the patient in the case of lung-cancer (conventional post-bronchoscopy, respiratory eco-endoscopy, thoracic, or pleural needle-aspiration), antibiotic inhalation therapy in the case of ronciectasias with no decompensation, and intensive treatment (nebulization, antibiotics, endovenous, etc.) in the remaining cases.
The implementation of the Day Hospital did not have a negative impact on any of the global indicators of service quality. On the one hand there was no increase in the number of readmissions during the period of the study, despite the increase in complexity already referred to. In fact the number of readmissions in relation to the number of patients attended to actually decreased. On the other hand, the number of deaths of hospitalized patients fluctuated during the period, with no clear trend either way.
DiscussionThe most relevant result of the present study is that it shows that the implementation of the Day Hospital specializing in the respiratory system increases the capacity and the quality of the care provided in a pulmonology service. This is probably due to a more precise adaptation of the services to the real needs of the population. The health-care requirements of the latter, and therefore the costs incurred, are increasing, so it is vital that the health-care systems adapt to this trend in order to remain both effective and efficient.
One of the most important premises in the search for new ways of delivering health-care is the need to reduce conventional hospitalization,15 which involves high costs, not only in terms of medical attention itself, but also in terms of hospital accommodation.15,16 In addition to this general need to reduce the occupation of hospital beds, there are often also more specific circumstances to take into account, such as intermittent building work, and the increasing need to isolate patients for one reason or another. As regards the medical costs associated with hospitalization, they primarily have to do with the need to attend to patients in high intensity areas, whether in terms of therapy or intensive care and/or supervision. Besides these considerations, there are also issues like the age and fragility of the patients, and the presence of comorbidities, factors which are increasingly problematic in our society. It is also necessary to take into account the costs incurred by the complications often associated with hosptalisation, such as colonization or infection by multiresistent germs,17 and deconditioning resulting from being confined to bed and/or from the reduction of normal, everyday activity. As regards hospital accommodation costs, the new system has not yet come up with plausible, cost-effective alternatives, as such expenses necessarily account for a large proportion of the total cost borne by any hospital.
This whole set of problems is what has given rise to the search for alternatives to conventional hospitalization. The ideas that have been explored include Day Hospitals, home-based hospitalization7,18–22 and short-stay and surveillance units, but it is Day Hospitals, whether general or specialized, that occupy a particularly prominent place. The appropriateness of one or other model probably depends on the characteristics of each hospital, and especially on its degree of tertiarism. In the particular case of and the treatment to the specific profile of each patient, as they often incorporate highly specialized instruments. As far as Pulmonology Day Hospitals are concerned, they would appear to be of particular value in supporting the process leading to the diagnosis of lung cancer.23 The use of such instruments in the Day Hospital setting can result in a four-fold increase in the efficiency of the care delivered to the patient, and therefore contribute to patient satisfaction.23 The treatment of COPD, or of the complications that often derive from this disease (e.g. colonization by multi-resistant germs), can also benefit from the clinical setting provided by the Day Hospital.20–24 Indeed it has been reported that this instrument can increase almost five-fold clinical efficiency in dealing with COPD exacerbations, and thus greatly improve the satisfaction of the patients treated in this way.23 Another pathology for which the Day Hospital is appropriate is bronchial asthma. Several different authors have shown that, given a careful selection of patients, it is possible to improve both the quality of the care delivered and the efficiency in the management of resources, and therefore also the satisfaction of the patients treated for asthma.23,25,26 Furthermore, the impact of a Day Hospital is not confined to its effectiveness in dealing with individual patients, but also has to do with the indirect overall effects it can have on the need for conventional hospitalization. It can lead to a reduction in the latter of up to 40%,27 which has huge implications for the reorganization of resources in pulmonology services.
Our work shows that since the early stages of the implementation of the Pulmonology Day Hospital, there has been a decline in the number of conventional hospital admissions. In our case, this was not due to a decrease in the pressure brought to bear on the pulmonology services as a whole, as the number of patients attended to was actually greater, but to a greater capacity for resolution. The same results are obtained when one analyses specifically the pathologies eligible for treatment in the Day Hospital setting. On the one hand, the number of admissions to hospital coincided with an increase in the complexity of the attention required, which suggests a more precisely targeted adaptation in the use of such a complex and expensive resource as hospitalization. As it has already been pointed out, these effects have direct repercussions in terms of cost, as the costs incurred by the Day Hospital are considerably less than conventional hospitalization,9 especially if the number of personnel involved is not increased unnecessarily. In the case that concerns us in this study, the staff was increased by one doctor and one nurse (morning shift only) to provide Day Hospital care, but one year later it was possible to reduce the conventional hospital ward-staff. The staff in question could be redeployed into new activities in other areas of the service.
Another interesting matter, albeit beyond the scope of the present study, is the fact that during the period of the study the number of complementary pulmonary examinations increased (Table 2). This is probably due to an increase in the overall complexity, and indicates that while Day Hospital care reduces the costs associated with hospitalization, it does not necessarily lead to a reduction in the intensity of diagnostic activity.
Viewed from a classical management perspective, the indicators of quality are primarily the number of readmissions and mortality.28 During the period of the present study, these indicators remained relatively stable and similar to those observed in previous years. Our results coincide with previous studies carried out in similar settings to ours, in which the implementation of Day Hospital systems, and the steady increase in their activity at the expense of conventional hospitalization, does not alter the number of readmissions or the overall patient mortality rate.29 It is also necessary to bear in mind the impact on the daily life of the patients as another indicator of quality in the process. While it is true that this is a more heterodox indicator from the management perspective, there can be no doubt that it is more relevant to the clinic and to the patient's perception. In this sense it is worth reflecting on the positive aspects of being able to offer medical attention which has less impact on the daily life of the patients and their families, enabling them to spend more time at home and in their familiar environments, and freeing up time for their own personal use, while at the same time reducing the risk of the adverse effects associated with hospitalization. Although the present paper does not include a study of the quality of life in relation to health-care and patient satisfaction, there is good reason to believe that the experience is regarded by patients as positive.23,25 This would be of particular importance for chronically ill patients or those suffering from cancer, for whom contact with the health-care system is frequent and can impact on other areas of their lives.
Our results cannot easily be compared with previous experiences of this kind in this country, on account of the heterogeneous conception of the system, and the period of time studied in each case. In the work of Golpe-Gómez et al., for example, a short period of time was used for the study, in a centre catering for a semi-rural population, and with a Day Hospital whose orientation was almost exclusively therapeutic.4 In this case, no reduction in the average length of hospitalization was observed, nor there was any change in the number of admissions in the pulmonology service, but this could be due to the short period of time during which the system had been in operation. As regards the more recent paper by Pomares et al., the study is more similar to our own, although the study period is longer. This study also shows a reduction in the pressure on casualty, in the number of hospital admissions, and in the length of hospitalization.30 Finally, the work of Sauret et al. refers to a period of time that is too remote from our own to enable us to establish any valid comparison.5
Besides the advantages already referred to in Pulmonology Day Hospitals, another consideration worth bearing in mind is the potential reduction in the pressure on casualty services. Many of the patients who access a specialized Day Hospital would have recourse to casualty if such a system did not exist. More often than not, the processes involved do not require only a single hospital, but usually require admission and the use of resources. In our centre, as in most other cases, around 90% of the patients admitted in the medical area come from casualty. This leads to the inevitable long waits, from the initial diagnosis to either improvement or hospitalization. It is common knowledge that such situations entail a negative impact on the quality of the care, and patients often find themselves being located in unacceptable circumstances during hours at a time. The possibility of a significant number of patients with respiratory disorders being treated in a Pulmonology Day Hospital setting is therefore extremely relevant. This system has a much more agile and focused management capacity, so that a high quality response can be delivered to meet the demand. It also has the capacity to adapt efficiently to changes in the demands made upon it. One typical example of this is the way in which the Day Hospital can increase the number of staff required or the attention timetables when demand peaks during the winter season. The cost entailed by these increases is relatively low, as it means taking advantage of an already existing infrastructure.
One important feature of the Pulmonology Day Hospital is its double-edged capacity for diagnosis and treatment. This gives it an advantage over its counterparts in cancer treatment and hematology, which are much more focused on treatment. The Pulmonology Day Hospital, not only provides treatment for patients with COPD exacerbations, asthma or interstitial illnesses, but also offers the possibility of rapid diagnosis where patients are suspected of suffering from pulmonary neoplasia, or neural effusion. In comparison with the surgical Day Hospitals, which have also become well established, medical Day Hospitals (not only pulmonology ones) have the advantage of not depending on another precarious resource, the availability of operating facilities. Viewed from a general perspective, all these advantages will together result in the appearance of more and more Day Hospitals specializing in pulmonology.
One somewhat disturbing result (and a very common phenomenon in the world of health care), is the absence of any kind of limitation in the demand. In fact, experience shows that any new system that is introduced ends up generating its own demand, in addition to the demand already existing prior to its implementation. In this case, the aim was to attend to the greatest possible number of patients with the least possible consumption of resources, without any loss of quality. It must be acknowledged that his aim has only been partially achieved, as, although occupation of hospital beds normally required for hospitalization could be reduced, demand is still increasing (in terms of the total number of patients) and the degree of complexity is also rising. In other words, although beds have been freed up and pressure on care and accommodation related resources has been relieved, there has been no parallel decrease in other types of consumption (e.g. drugs and administrative or diagnostic stationery) or in the number of doctors and nurses required. It is common knowledge that any intervention that renders a hospital more effective entails all the more activity and, consequently, more growth. Although the costs per unit might well be lower, they will result in an increased final cost. Given the current payment systems in the public health service, even if the social value of health care increases, this will not translate into greater revenues for the hospital that provides such care.
Currently, and across a range of institutions, other care-oriented instruments are being developed, such as specialized short-stay units or home-based hospitalization. These systems are not necessarily alternatives to Pulmonology Day Hospitals, but can be complementary. They will share the limitations of the Day Hospital already outlined in the previous paragraph. For this reason, an interesting management alternative in the care of patients with respiratory disorders would be an improvement in the effectiveness of a series of mobile care systems (Table 2). Both an improved attention on the part of the general practitioner and the external pulmonologist would help to reduce the pressure on hospitals. In this sense, linking activity of the external pulmonologist to the equivalent service in the hospital within his or her catchment area (Specialised Care Reform or SCR, Fig. 1 and Table 2) could contribute to helping and homogenizing diagnostic and therapeutic procedures, thus making the services required from the hospital more agile.
Limitations of the Study and of the Day HospitalOne potential limitation of the present study is the fact that not all respiratory patients are examined within the Pulmonology Service. Other services of internal medicine, medicine of infectious diseases, cardiology and Casualty have probably been able to deal with illness episodes suffered by these patients. The present study has limited itself to analysis within the specific field of pulmonology. Finally, on account of their complexity, it has not been possible to analyse the impact of the Day Hospital on the overall activity in casualty services. The diversity of the types of attention required by patients with respiratory problems in this area makes it difficult to obtain reliable data.
To sum up, the present study demonstrates the positive effects of setting up a Day Hospital specializing in Pulmonology. The greater efficiency in the management of patients with respiratory disorders seems to have an impact not only on the management of the service itself, but also on the general running of the hospital and on the patient. In view of the scarcity of studies dealing with the impact of Day Hospitals on the management of pulmonological services, there is a pressing need to gather data from our cumulative experience of such systems.
Conflict of InterestsThe authors declare having no conflict of interests.
The authors thank Dr. Cristina Iniesta, for her determined support in favor of the creation of the Pulmonology Day Hospital, and Sergi Mojal, of the AMIB (IMIM) for his methodological support in the statistical analysis.
The last two authors share equivalently the position of senior author.
Please cite this article as: Cots F, et al. Hospital de día: análisis de resultados, costes y asignación de recursos en neumología. Arch Bronconeumol. 2013;49:54–62.
This study has been the central work of the Advanced Studies Diploma (DEA) Jaume Raventós at Universitat Autònoma de Barcelona.




www.publicationethics.org.




Archivos de Bronconeumología follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals