


Surgical treatment of thoracic inlet tumors represents a challenge to the surgeon due to its location and anatomical elements contained in that region. Several surgical approaches have been proposed, each of them showing some advantages but drawbacks as well. In our opinion, the anterior transmanubrial approach described in 1997 is one of the most convenient approaches. The objective of this paper is to describe and comment on some technical aspects of the procedure in order to aid surgeons who intend to perform this surgical approach. Moreover, we show our results in five patients and also comment on other approaches in this pathology.
El tratamiento quirúrgico de los tumores del estrecho torácico superior supone un reto para el cirujano por su localización y por los elementos anatómicos que contiene dicha región. Se han propuesto varias vías de abordaje y cada una de ellas presenta ventajas e inconvenientes. En nuestra opinión, el abordaje anterior transmanubrial descrito en 1997 es uno de los más adecuados. Realizamos la descripción y comentarios sobre algunos detalles técnicos como ayuda al cirujano que pretenda realizar este abordaje, mostramos nuestros resultados sobre 5 pacientes y comentamos asimismo otros diferentes abordajes para esta patología.
Tumors of the superior thoracic aperture are a challenge for surgeons because their location is difficult to access as they are hidden by the clavicle and ribs and also because they are close to important vascular and nervous structures of the head and upper extremities.1 Several accesses have been proposed to approach their treatment,2–5 and each has advantages and disadvantages. In our opinion, the anterior transmanubrial approach described in 19975 is one of the best. In this text, we intend to describe the technique and provide comments about some of the technical details as an aid to surgeons who plan to perform this approach. We will also provide our own results.
Description of the TechniqueThe patient is placed in supine decubitus position with the upper limb in abduction (the elbow is slightly flexed in order to avoid nerve lesions due to forced stretching) of the side to be operated on and with a retroscapular cushion. The head is turned 45–60° toward the contralateral side and the field is prepared: neck, anterior thorax and deltopectoral region.
The skin incision is L-shaped on the left-hand side, while it is an inverted L on the right-hand side. In both instances, the angle is rounded to favor the final skin suture. The vertical branch is done medial to the sternocleidomastoid (SCM) muscle and the horizontal one runs caudal to the clavicle for some 2cm and is then lengthened up to the deltopectoral fold (Fig. 1). The surgeon stands on the side of the skin incision. Once the subcutaneous cell tissue is dissected, the muscle dissection is completed as follows: following the most anterior edge of the SCM muscle at the height of the larynx until its insertion in the sternum, this muscle is retracted laterally in order to access the internal jugular vein; it is marked with a vessel loop and serves as a guide to identify its union with the ipsilateral subclavian vein and to locate the contralateral brachiocephalic vein. The pectoralis major vein is dissected, separating its muscle fibers horizontally with the help of scissors and electrocoagulation, and an autostatic retractor provides exposure of the subjacent minor pectoral muscle (Fig. 1). The minor pectoral is dissected easily using a thick dissector clamp or simply with a finger, keeping in mind that underneath are the subclavian veins leading to the axilla. Once dissected, the fat covering the axillary vessels and the branches of the brachial plexus is dissected. In this manner, distal vascular control is achieved (Fig. 1). Afterwards, an L-shaped incision of the sternal manubrium is made with the sternotomy saw after ligating the internal mammary blood vessels. The horizontal cut over the manubriosternal is in the first intercostal space, meaning that the manubrium is cut between the first and second ribs. Then, costotomy is done on the first rib at 1.5–2cm from the cut manubrium; this initiates the elevation of the osteomuscular flap formed by the SCM muscle, the clavicle, a small part of the first cut rib that is adhered to the cut manubrium, and the cut sternal manubrium. Nonetheless, the most difficult moment is when the clavicle is separated from the first rib, cutting the firm costoclavicular ligament. In order to do so, it is more comfortable if the surgeon changes places and stands on the contralateral side of the incision to have a direct frontal in a more ergonomic position (Fig. 2). The venous vascular plane is the most anterior and superficial, and following the dissection of the internal jugular vein and its union with the subclavian vein is a good guide or reference point to cut the cited ligament and avoid any iatrogenic vascular injury. Small collateral venous branches may appear, which can be ligated. As the costoclavicular ligament is cut, the assistant pulls the osteomuscular flap up with a cord, raising the cut manubrium joined with the clavicle in order to make for better viewing and widen the surgeon's field (Fig. 2). The field is exposed and the following stage of the intervention is begun, which includes evaluating the extent of the lesion, dissecting it and determining what structures are affected in order to then carry out the resection and a possible vascular reconstruction if necessary. The resection of the innominate vein does not require reconstruction. In the post-operative period, the patient may present edema of the upper limb, but this is usually temporary (some days or weeks) if it is kept high, wrapped in elastic bandages, and with the aid of massages or physiotherapy. For the arterial reconstruction, a PTFE prosthesis (number 6–8 depending on the caliber) is usually used after the vascular clamping and prior to intravenous heparinization (0.5mg/kg).

Position of the patient in order to perform the skin incision: upper limb is in abduction and the neck is rotated 45–60° toward the contralateral side. Detail of the distal control of the subclavian vessels using the separation of the muscle bundles of the pectoral mayor with an autostatic retractor and the posterior section of the minor pectoral muscle.
. Diagram of the cranial and lateral traction after cutting the costoclavicular ligament, elevating the osteomuscular flap and exposing the subclavian vessels (proximal and distal control).")
Detail of the costoclavicular ligament being severed to allow for the osteomuscular flap to be elevated, separating the clavicle and the sternocleidomastoid muscle from the first rib and the underlying subclavian vessels. The surgeon is on the opposite side from the initial incision in order to have a direct view and a more ergonomic position (the surgeon changes place). Diagram of the cranial and lateral traction after cutting the costoclavicular ligament, elevating the osteomuscular flap and exposing the subclavian vessels (proximal and distal control).
The closure of the wound is quick and easy. Osteosynthesis of the sternal manubrium is carried out with 2 steel sutures, or instead with titanium plates (Sternalock®, Walter Lorenz Surgical, Jacksonville, FL, USA). The major pectoral muscle, subcutaneous cell tissue and skin are closed after leaving in cervical and thoracic drains.
If there was a lung tumor involved, lobectomy carried out through the described approach could be difficult and/or uncomfortable, although not impossible. To do so, once the apical tumor is freed from the structures that it affects, the wound is closed and thoracotomy is done as usual and according to the preferences of each surgeon (posterolateral, anterolateral muscle-sparing or video-assisted thoracoscopy).
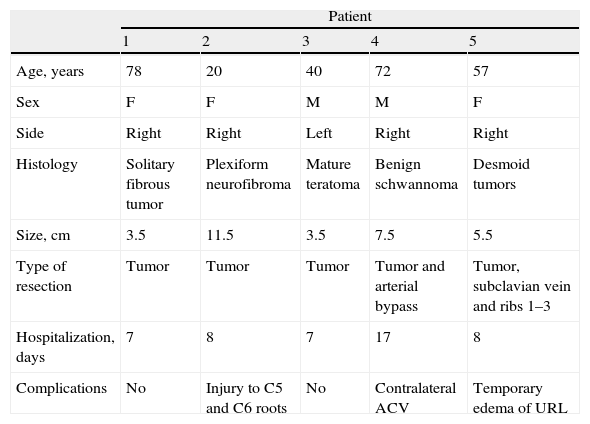
ProcedureIn our experience, we have performed this approach in 5 patients between 2008 and 2011. Four cases were on the right side and one on the left (Table 1).
Characteristics of the Patients With Anterior Transmanubrial Approach.
| Patient | |||||
| 1 | 2 | 3 | 4 | 5 | |
| Age, years | 78 | 20 | 40 | 72 | 57 |
| Sex | F | F | M | M | F |
| Side | Right | Right | Left | Right | Right |
| Histology | Solitary fibrous tumor | Plexiform neurofibroma | Mature teratoma | Benign schwannoma | Desmoid tumors |
| Size, cm | 3.5 | 11.5 | 3.5 | 7.5 | 5.5 |
| Type of resection | Tumor | Tumor | Tumor | Tumor and arterial bypass | Tumor, subclavian vein and ribs 1–3 |
| Hospitalization, days | 7 | 8 | 7 | 17 | 8 |
| Complications | No | Injury to C5 and C6 roots | No | Contralateral ACV | Temporary edema of URL |
F, female; M, male. ACV, cerebrovascular accident; URL, upper right limb.
Simple tumor resection was performed in 3 cases. In addition, one case required resection of the subclavian vein together with 3 ribs en bloc, and another case required the implantation of a lateral-terminal PTFE-6 prosthesis between the innominate artery and the subclavian artery in a patient who had been operated on 2 previous times with incomplete resection and tumor relapse (patient 4). The bypass was applied as a prophylactic measure because the subclavian artery suffered total occlusion after previous surgeries and developed irrigation of the upper right limb that was mainly a detriment to the arterial branches of the internal mammary artery, which is cut in this approach. This patient had a contralateral cerebrovascular accident during the immediate post-op, which was apparently unrelated with the surgical technique, but the patient is currently asymptomatic. There were no complications related with the surgical wound, nor were there any thoracic deformities in any of the cases. Patient 2 experienced injury to the C5 and C6 nerve roots, probably due to the fact that tumors that originate in the nerves (in this case, von Recklinghausen disease) may be functional and their exeresis may cause neurological deficiencies.
CommentsSeveral approaches have been reported for thoracic inlet tumor surgery. These tumors can be cervical–mediastinal, in the thoracic wall or the apex of the lung (Pancoast–Tobias tumor).6,7 Each approach presents advantages and disadvantages that all surgeons who perform these operations should know, apart from being familiarized with the cervical and thoracic anatomical structures. Currently, there is no consensus about which is the best access pathway for approaching tumors that are located anteriorly, although in posterior cases the Shaw–Paulson–Lee method is more consolidated.8
The first group to describe an anterior approach for treating anterior apical tumors was Masaoka et al.2 in 1979 by means of the anterior trans-sternal pathway, which included proximal mid-sternotomy extended to an anterior thoracotomy at the fourth intercostal space and another cervical horizontal extension above the clavicle. This approach, however, does not provide good access or control of the distal subclavian vessels, brachial plexus, back of the ribs, transverse apophysis or of the vertebrae if they are affected by the tumor.
Later, Dartevelle et al.3,4 described the anterior transclavicular approach, used by French vascular surgeons to access the subclavian artery,9 which entails resection of the internal half of the clavicle for controlling the subclavian vessels and those of the brachial plexus. This novelty opened the door for treatment with complete resection of tumors that are anterior to the apex and invade difficult-to-control vascular and nerve structures. This option, however, presents the disadvantage of the esthetic defect of bone resection, clavicle instability and, if the long thoracic nerve is injured during thoracotomy, there could be a winged scapula over a sectioned clavicle with no stability or impeded displacement of the scapula and upper limb.
In 1994, Tatsumura et al.10 described an approach with a large incision that was initiated above the 2nd to 3rd thoracic spinal apophysis, going around the scapula caudally and curving up to the height of the mammilla, or rather with prolongation up to the sternoclavicular articulation if there were a need to control the subclavian vessels. This approach allows for the evaluation of the posterior and anterior lung apex, but many muscles are severed (trapezius, rhomboids, serratus major, and pectorals) and there may be difficulty for moving the upper limb during post-op, or even muscular atrophy if innervation is compromised.
The hemi-clamshell or trapdoor method11 is also another valid alternative because it provides control of the mediastinum or lung, although it does not provide adequate vision of the distal subclavian vessels or of the brachial plexus. However, there are reports of vertebral resections due to tumor invasion using this approach.12
The anterior transmanubrial approach was described by Grunenwald and Spaggiari5 in 1997. It offers the advantages of the approach proposed by Dartevelle et al.3 but it leaves the clavicle and SCM muscle intact (as explained in the technical description), and therefore does not result in destabilization of the mobility of the upper limb or any sort of esthetic defect. Other variations have also been described with some modifications entailing the deinsertion of the sternoclavicular joint in order to traction the clavicle caudally, move it away from the thoracic operculum and access the subclavian vessels and the brachial plexus,13 or a mini trapdoor14 or a section of the sternum to widen the cervical field.15 The anterior transmanubrial approach also provides access to the spinal column from C3–T3 in cases of invasion.5,16
Indications and LimitationsThere may be several indications for this approach: cervical–mediastinal tumors (benign, malignant), tumors of the pulmonary sulcus (Pancoast–Tobias tumor) and the chest wall (first rib and clavicle), infections of the pulmonary vertex or osteomyelitis of the first rib or the sternoclavicular joint, vascular pathology of the subclavian vessels and surgery of the cervical column or upper thorax.
It is not always necessary to widen the incision up to the deltopectoral groove or to dissect all the structures, as previously explained. The incision can be adapted to the situation according to the pathology and the preoperative images in order to either limit the exposure or instead to extend it according to the intraoperative findings.16 There are different approaches for anterior cervical–thoracic tumors, with some variations between them. We believe that the anterior transmanubrial method offers an excellent work field with control of the subclavian vessels, brachial plexus, exposure of the cervical and upper dorsal column and easy reconstruction with good esthetic and functional results. The application of other similar approaches may be useful according to the type of intervention proposed, its location, etiology and the structures that are invaded.
Conflict of InterestsThe authors declare having no conflict of interests.
Please cite this article as: Honguero Martínez AF, et al. Aspectos técnicos del abordaje anterior transmanubrial en la cirugía de los tumores del estrecho torácico. Arch Bronconeumol. 2012;48:419-22.







