
The CA 19.9 antigen is a glycoprotein synthesized in several epithelia that is typically high in the serum of patients with pancreatic tumors. Thus, levels above 300U/l have a positive predictive value of about 90%.1 Other tumors (bile duct, gastric, colon, hepatic, ovarian, endometrial, pulmonary, or urothelial) or different benign processes (hepatitis, cirrhosis, cholangitis, cholecystitis, pancreatic pseudocyst, pancreatitis, pulmonary fibrosis, bronchial asthma, asbestosis, bronchiectasis, tuberculosis, renal failure, mucinous cysts, hydronephrosis, Sjögren's syndrome, rheumatoid arthritis, erythematous lupus, dermatopolymyositis, or giant cell arteritis2–4) may also run their course with high serum CA 19.9 levels (in the latter case, with more moderate values).
Increased serum levels of CA 19.9 in lung tumors, especially in adenocarcinomas, are a known fact, although uncommon.5–7 Therefore, we consider it interesting to discuss 4 cases of pulmonary non-small-cell carcinoma treated in our unit within the last 2 years. The notably high CA 19.9, especially in 2 of the patients, made the initial suspected diagnosis lean toward digestive tumor processes.
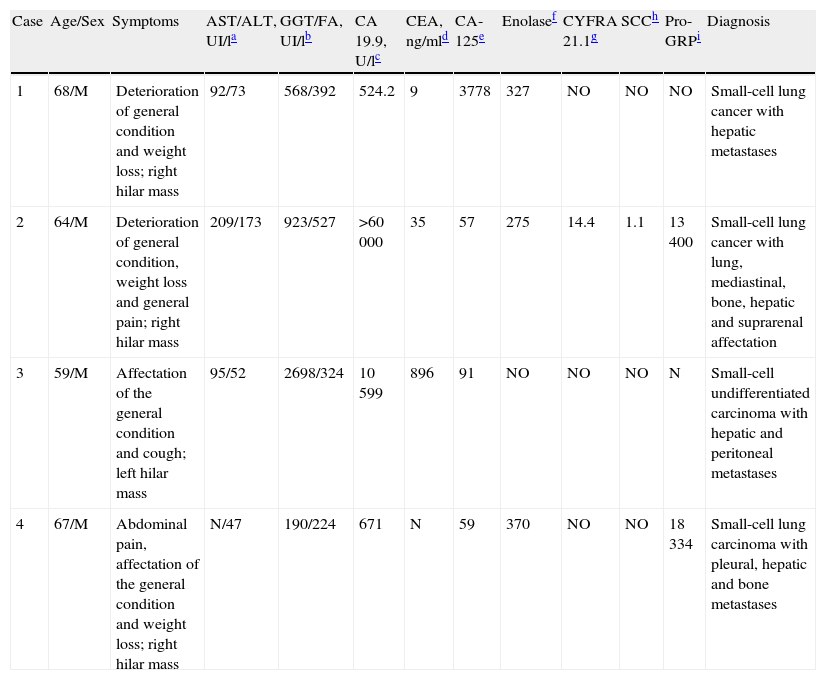
In the time period, we treated 4 males, all with important smoking histories, non-small-cell lung cancer and CA 19.9 values higher than 300U/l. Mean age was 64.5 (SD, 4.01), and general patient characteristics are shown in Table 1.
Characteristics of Patients With High CA 19.9.
| Case | Age/Sex | Symptoms | AST/ALT, UI/la | GGT/FA, UI/lb | CA 19.9, U/lc | CEA, ng/mld | CA-125e | Enolasef | CYFRA 21.1g | SCCh | Pro-GRPi | Diagnosis |
| 1 | 68/M | Deterioration of general condition and weight loss; right hilar mass | 92/73 | 568/392 | 524.2 | 9 | 3778 | 327 | NO | NO | NO | Small-cell lung cancer with hepatic metastases |
| 2 | 64/M | Deterioration of general condition, weight loss and general pain; right hilar mass | 209/173 | 923/527 | >60000 | 35 | 57 | 275 | 14.4 | 1.1 | 13400 | Small-cell lung cancer with lung, mediastinal, bone, hepatic and suprarenal affectation |
| 3 | 59/M | Affectation of the general condition and cough; left hilar mass | 95/52 | 2698/324 | 10599 | 896 | 91 | NO | NO | NO | N | Small-cell undifferentiated carcinoma with hepatic and peritoneal metastases |
| 4 | 67/M | Abdominal pain, affectation of the general condition and weight loss; right hilar mass | N/47 | 190/224 | 671 | N | 59 | 370 | NO | NO | 18334 | Small-cell lung carcinoma with pleural, hepatic and bone metastases |
Except in one of the cases, the clinical presentation included severe deterioration of the patients’ condition, with very striking cholestasis and hepatomegaly. This, together with high CA 19.9 levels (in all 4 patients above 500U/l, and above 10000U/l in 2) meant that the initial suspected diagnosis did not coincide with the definitive diagnosis. In the 4 cases, abdominal computed tomography (CT) ruled out pancreatic masses. Meanwhile, neuron-specific enolase (determined in 3 patients) was clearly high, as was pro-gastrin-releasing peptide (Pro GRP), with values that were 200 times above normal. The poor survival in the 4 patients (just 16 weeks on average) reflected the advanced clinical state at presentation.
Tumor markers are substances that are produced or induced by either a tumor or by the surrounding tissues.8 They have limited specificity and sensitivity, although they are of interest in tumor diagnosis. Their main application resides in follow-up, in the evaluation of treatment efficacy and in prognosis.
Neuron-specific enolase, Pro GRP, squamous cell carcinoma (SCC) antigen, or CYFRA 21.1 are markers that are usually used when given the suspicion for lung cancer (small-cell in the first 2 cases or epidermoid in the remainder). Nevertheless, publications in the medical literature about the management of this entity do not recommend the systematic use of tumor markers due to their very limited efficacy, and they hardly even mention CA 19.9, which is not considered useful in this context.9,10
CA 19.9 is present in the glands of bronchi and bronchioles. It is therefore plausible (although immunohistochemistry techniques are not done) that the origin of their increased level is the neoplastic bronchiolar epithelium,7 regardless of the potential impact of the hepatic metastasis in all the reported cases.
It can thus be deduced that CA 19.9 may present higher levels in small-cell lung cancer, although its determination is not considered clinically useful. This consideration may be useful in order to properly interpret analytic and imaging results in this context.
Please cite this article as: Prieto De Paula JM, et al. Carcinoma microcítico de pulmón y elevación del marcador tumoral CA 19.9. Arch Bronconeumol. 2012;48:385–6.







