







Chronic obstructive pulmonary disease (COPD) is a common respiratory condition and one of the leading causes of death. Our aim was to analyze the association between emergency room visits due to this disease and meteorological variables and atmospheric contaminant levels in Santander, depending on the origin and trajectory of air masses.
MethodsData from emergency room visits at Hospital Marqués de Valdecilla were collected on a daily basis during an 8-year period. Data on concentrations of the main atmospheric pollutants and meteorological variables were also recorded. Retrotrajectories leading to Santander at a height of 1500m above sea level were then calculated. Finally, a correlation model was produced to evaluate the effect of the contaminants on emergency visits due to COPD.
ResultsThere is a direct association between PM10 levels and the number of visits to the emergency room due to COPD. For every 10μg/m3 increase in pollutant levels, emergency visits increase by3.34% (P=.00005), and this effect is enhanced in individuals over 74 years of age. This effect is heightened when PM10 levels depend on air masses from the South and when air recirculation occurs. There is no association between other pollutants and the number of visits to the emergency room.
ConclusionsExposure to high levels of PM10 causes exacerbations in COPD patients. By studying the atmospheric circulation pattern, we can predict whether PM10 levels will be inappropriately high, and we can also obtain information about the particle components.
La enfermedad pulmonar obstructiva crónica es una enfermedad de alta prevalencia y una de las principales causas de muerte a nivel mundial. El presente trabajo analiza la relación de esta enfermedad con las variables meteorológicas y los niveles de contaminantes atmosféricos en Santander, atendiendo al origen y trayectoria de las masas de aire.
MétodosSe recogieron datos diarios de visitas a urgencias en el Hospital Marqués de Valdecilla de un periodo de 8 años, así como la concentración de los principales contaminantes atmosféricos y de las variables meteorológicas. Posteriormente se calcularon las retrotrayectorias con destino en Santander, a una altura de 1.500m sobre el nivel del terreno. Finalmente, se elaboró un modelo de correlación para evaluar el efecto de los contaminantes sobre las urgencias por EPOC.
ResultadosExiste una asociación directa entre los niveles de PM10 y las urgencias por EPOC. Por cada 10μg/m3 de aumento del contaminante, las urgencias incrementan un 3,34% (p=0,00005), y el efecto se intensifica en las personas mayores de 74 años. Cuando los niveles de PM10 son dependientes de masas de aire procedentes del Sur, así como ante situaciones de recirculación, el efecto es mayor. Con el resto de contaminantes la relación con las urgencias no es estadísticamente significativa.
ConclusionesLa exposición a PM10 provoca descompensaciones en los pacientes con EPOC. Atendiendo al patrón de circulación atmosférica se puede estimar si los niveles de PM10 van a ser elevados, y también se obtiene información sobre los componentes de las partículas.
Chronic obstructive pulmonary disease (COPD) is a highly prevalent condition that affects about 10% of adults over 40 years of age, and is one of the leading causes of death worldwide.1,2 The pathogenesis of COPD has been linked to a chronic inflammatory response of the airways and lungs to noxious particles and gases,3,4 generally related to smoking. Several factors that contribute to the development of the disease or the onset of exacerbations in COPD patients have been identified,5,6 and much progress has been made in the last decade in understanding the effect of poor air quality on the mortality and morbidity associated with this disease.7–9
Most pollutants enter the body via the airway, which is why the effects of poor air quality on the respiratory system are particularly notable. Contaminants cause inflammation of the respiratory system, saturate decongestion pathways, and alter tissue repair and immune defence systems.10
Small diameter particulate matter (PM10) aerosols are among the most widely studied air pollutant compounds in healthcare. Epidemiological studies have shown that exposure to high particulate matter (PM) concentrations is associated with COPD,11,12 and experimental studies have described certain physiopathogenic mechanisms that could explain this association: changes in the diffusing capacity of the lungs for carbon monoxide, alterations in oxygen saturation and increase in inflammatory markers together with increased autophagy.13
Although the relationship between high levels of PM and different diseases has been described, little is known about the impact of the composition of PM on health. The composition of PM varies according to both the area studied (for example, high concentrations of carbonaceous particles are found in industrial areas with high traffic density, such as Madrid or Puertollano, while marine aerosol levels are especially high on the Atlantic coast)14 and atmospheric dynamics,15 so the effects of PM will vary in terms of time and space. The analysis of atmospheric dynamics provides information on the origin of air masses, showing the source of aerosols and their evolution over time. This data can be used to determine the presence of additional sources of atmospheric pollution and estimate the composition of the particulate matter.
This study has 2 objectives: first, to analyze the relationship between emergency visits to the Hospital Universitario Marqués de Valdecilla for COPD and meteorological variables and the levels of the main atmospheric pollutants (nitrogen dioxide [NO2], carbon monoxide [CO], sulphur dioxide [SO2], ozone [O3] and PM10) in the city of Santander, a coastal city with little industrial activity; and second, to determine whether the incidence of PM10-related COPD emergencies varies according to the origin and trajectory of air masses.
MethodsWe performed a retrospective correlation study between 2003 and 2010 to analyze the relationship between emergency visits for COPD at the University Hospital Marqués de Valdecilla, a tertiary hospital in the city of Santander, and different environmental variables calculated on a daily scale.
Emergency Room VisitsAnonymous data from emergency visits for COPD were collected by the Admission and Documentation Service of the Hospital Universitario Marqués de Valdecilla (HUMV).
The reasons for emergency consultation at the HUMV are not assigned a code; instead, the diagnostic impression of the attending physician is recorded using the words or abbreviations that, in their opinion, best define the patient's disease or symptomatology. In the case of COPD, the terminology used varies greatly (“chronic bronchitis”, “pulmonary emphysema”, “chronic bronchopathy”, “bronchial exacerbation”, “chronic bronchopneumonia”, among others). In other words, there is no definitive, coded diagnosis (as is the case with ICD codes used on hospital admission forms). This means that in order to collect data on COPD emergencies from the hospital's emergency room database, we first had to filter the records using symptoms and terms that can be used to describe the disease, and then examine each record individually.
All emergency visits for COPD were collected, irrespective of whether or not they culminated in hospitalization.
Atmospheric Pollutants and Meteorological VariablesDaily data for the main atmospheric pollutants (CO, NO2, O3, SO2 and PM10) in the city of Santander were collected. There are 3 types of air quality measurement stations in the city: urban background, traffic and industry. Urban background stations provide the most comprehensive information about the air to which most of the population is exposed, and are therefore the best source of information for epidemiological studies. In this study, we worked with data from the Tetuán fixed measurement station, for various reasons: it measures urban background, it is located in the centre of the city next to the HUMV, and it has the most comprehensive series of pollutants in Santander for the study period. The data were obtained from the Centre for Research and Environment (CIMA, in its Spanish acronym) of Cantabria and were cleaned and validated by eliminating manifestly incorrect records.
We also included a series of daily meteorological variables: maximum wind speed, average daily humidity, maximum, minimum and average temperature, maximum and minimum pressure, precipitation volume, and global solar radiation. This data was obtained from the Santander-Parayas measuring station, which contains the most comprehensive historical series within the city. The meteorological data were obtained from the Spanish Meteorological Agency (AEMET, in its Spanish acronym).
Back-TrajectoriesThe origin and trajectory followed by particulate matter before it reached the study area were obtained using atmospheric back-trajectories. A back-trajectory shows the path taken by an air mass before it affects a certain area, and gives a clearer picture of the synoptic weather conditions in a given region. Back-trajectories can also be used to interpret the evolution of air quality levels, since they can distinguish between external and local inputs. In this study, we calculated the daily 96-h back-trajectories at a height of 1500m above sea level in the city of Santander at 12 noon UTC. The physical and geographic magnitudes of each back-trajectory were calculated by running a dispersion model (HYSPLIT, http://ready.arl.noaa.gov/HYSPLIT.php) using meteorological files from the FNL database, managed by Air Resources Laboratory.
In a second phase, the trajectories were grouped into a small number of categories according to their length and latitude at consecutive 1-h intervals.16,17 The K-means clustering algorithm was used with the Euclidean distance metric.18 Following the example of other studies, and due to the need to reduce the number of samples used in subsequent analyses, we defined a total of 6 trajectories.
Statistical AnalysisA Poisson regression model was created to evaluate the association between the environmental variables and the emergency room visits for COPD, in which the dependent variable was emergency visits, the covariables were seasonality and trend, and the predictor variables were the effect of atmospheric pollutants (in aggregate and as individual compounds) and the meteorological variables described above.
In the case of PM10, as it was the only compound with a statistically significant association, the cumulative effect was evaluated by adding a new variable (the sum of PM10 levels on a specific day plus those of the 2 previous days).
To analyze the association of PM10 according to the back-trajectory, a new “virtual” variable was created for each atmospheric situation that contained pollutant levels on the days with that type of weather, and 0 for other days.
Finally, in pollutants for which an association was found, the Student's t-test was used to determine whether the number of hospital visits for COPD differed according to whether the atmospheric compound was above or below the threshold levels established by the WHO and in current regulations.
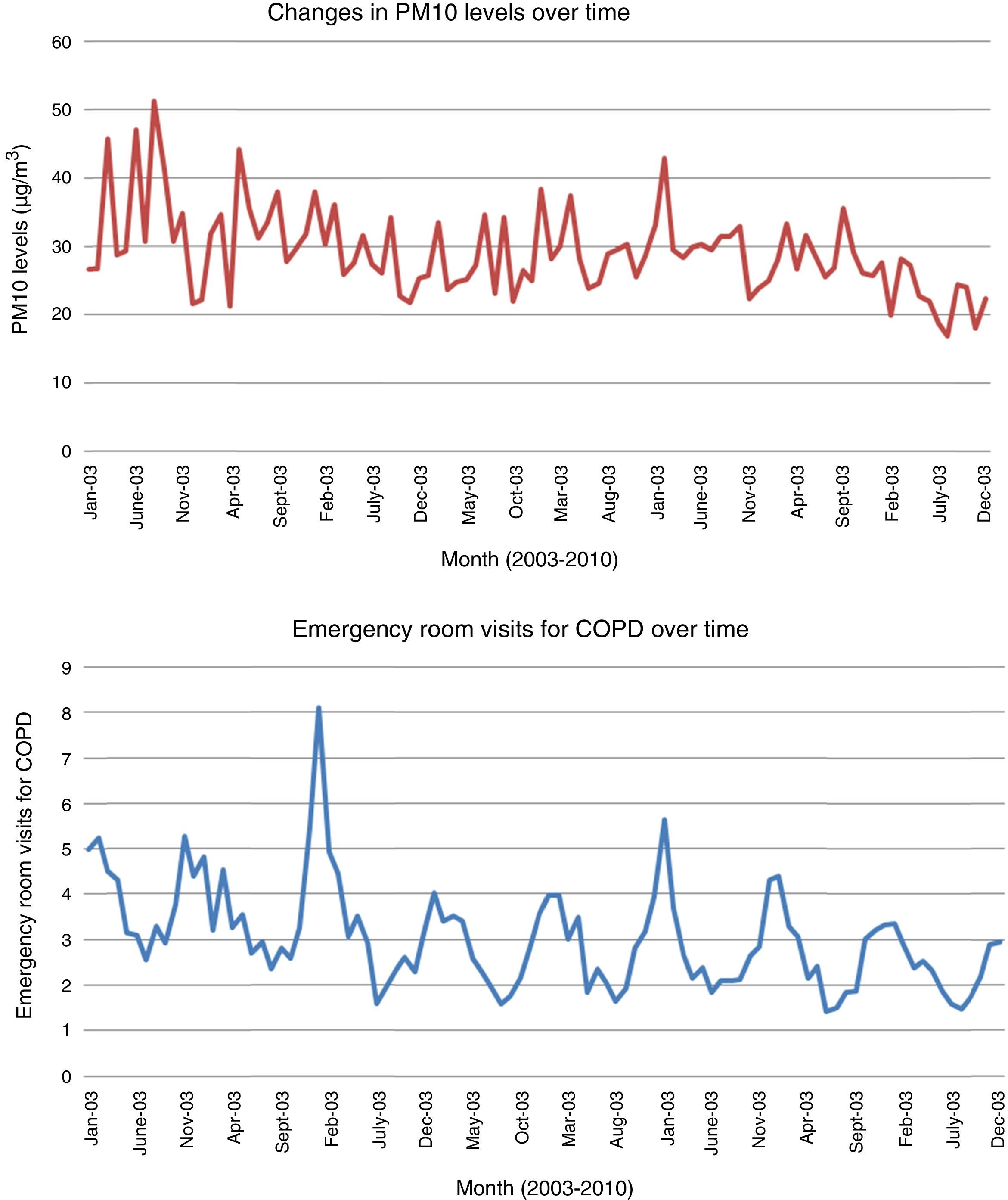
ResultsEmergency Room Visits for Chronic Obstructive Pulmonary Disease in Cantabria and Their Association With Environmental VariablesDuring the 8-year study period, 8861 episodes of COPD were treated in the emergency department of the HUMV, with hospitalizations peaking in a cyclic pattern (Fig. 1). Nearly all (98%) visits for this disease corresponded to individuals aged 44 years or older, and 50% corresponded to those aged over 74 years.
The analysis of the association between environmental variables and emergency visits for COPD in the HUMV showed an association between PM10 exposure levels and hospital visits for this disease. No significant associations were found with the remaining meteorological variables or with other study pollutants.
The results show that emergencies increased by 3.34% for every 10μg/m3 increase in PM10 levels (P=.00005), and by 3.75% in individuals aged of 74 (P=.001).
The analysis of the effect of the accumulated concentration in the 2 days prior to the emergency visit also showed a statistically significant relationship (P=.001), albeit with less effect, insofar as emergency visits increased by 1% for every 10μg/m3 increase in accumulated PM10 levels.
When emergencies were analyzed according to whether PM10 levels exceeded or met the WHO threshold for health protection19 − the daily limit is 50μg/m3 − the t test showed that COPD patients presented significantly more decompensations on days when PM10 levels were higher than 50μg/m3 vs days when levels were below this value (P=.0005). Our results show that in Santander, 18.5% more patients on average were treated on days when PM10 levels exceeded the WHO threshold (Fig. 2).
Characterization of the Aerosol Load According to trajectory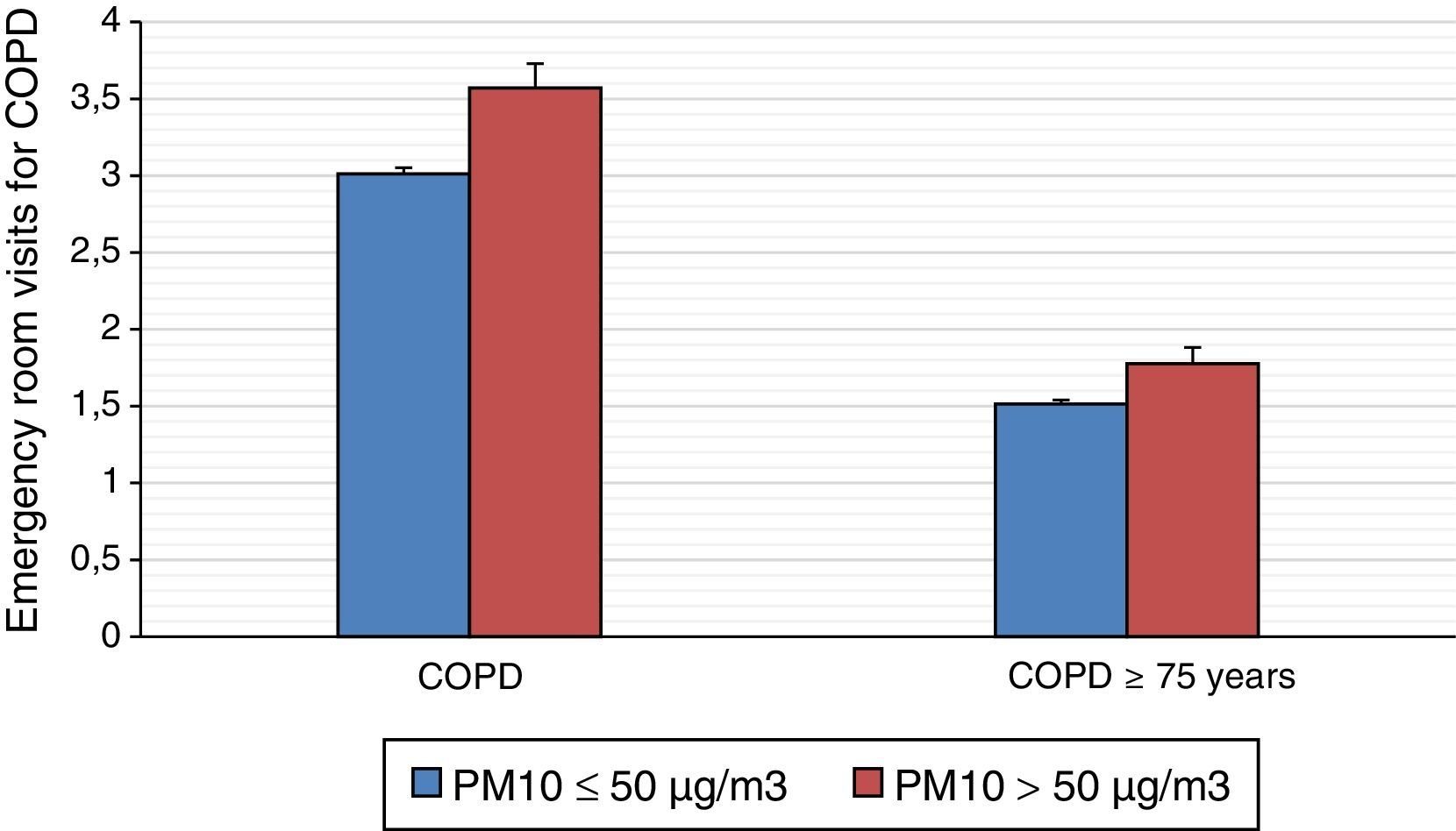
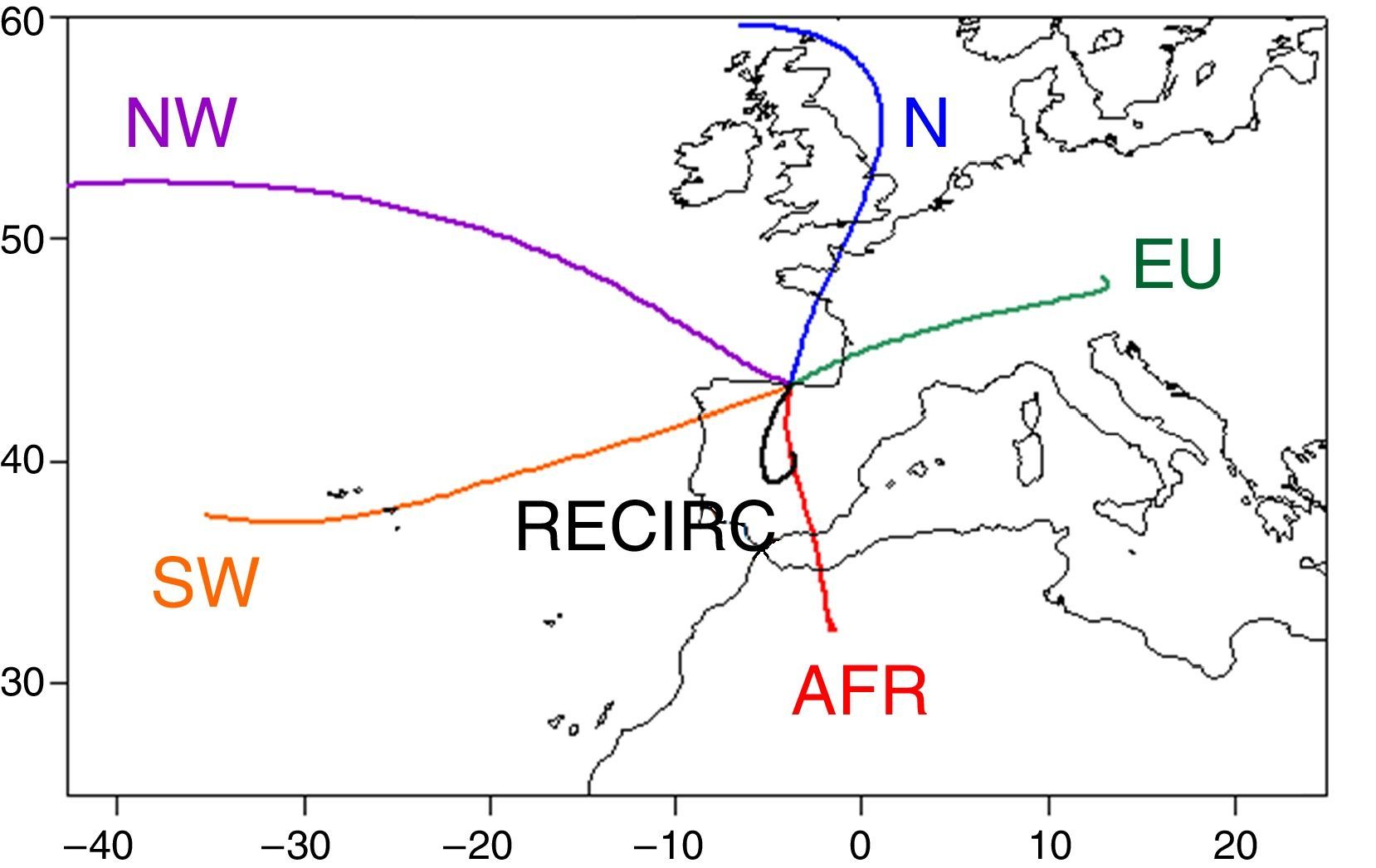
The average trajectory of each category (named according to the area covered before reaching Santander) is shown in Fig. 3. The trajectories from the Atlantic Ocean (NW and SW) are the most frequent (68%), as would be expected of a climate that for much of the year is under the influence of the Westerlies. This origin suggests a low aerosol load, with a predominance of marine aerosols and a low anthropogenic load. The European (EU) and African (AFR) trajectories, however, are continental. The N trajectory travels over the Atlantic Ocean, although the last sections cross the British Isles and France. Finally, a small number of slow-moving trajectories (RECIRC, recirculation) are found. These are typical of summer weather and cause the high temperatures found in the flat, open plains of central Spain.
The most striking element of the mean PM10 load of each trajectory is the contrast between the essentially oceanic (SW, NW, N) and continental (RECIRC, AFR, EU) trajectories, the first being much “cleaner” than the latter (Fig. 4). In addition, certain singularities can be detected within each group. For example, in the case of “oceanic” air masses, the N trajectory tends more towards the high percentiles, probably as a result of picking up anthropogenic aerosols as it travels over the British Isles or Western Europe. The African trajectory has the highest PM10 load, but peak PM10 levels have occasionally been identified in European trajectories. PM10 levels are also high in recirculation trajectories. This is because stagnation prevents the renovation of air masses, which then absorb increasing amounts of particulate matter from re-suspended pollutants from population centres in the interior of the peninsula and from the resulting secondary aerosols.20,21
Association Between Episodes of Chronic Obstructive Pulmonary Disease and PM10 Levels According to the Origin and Trajectory of Air Masses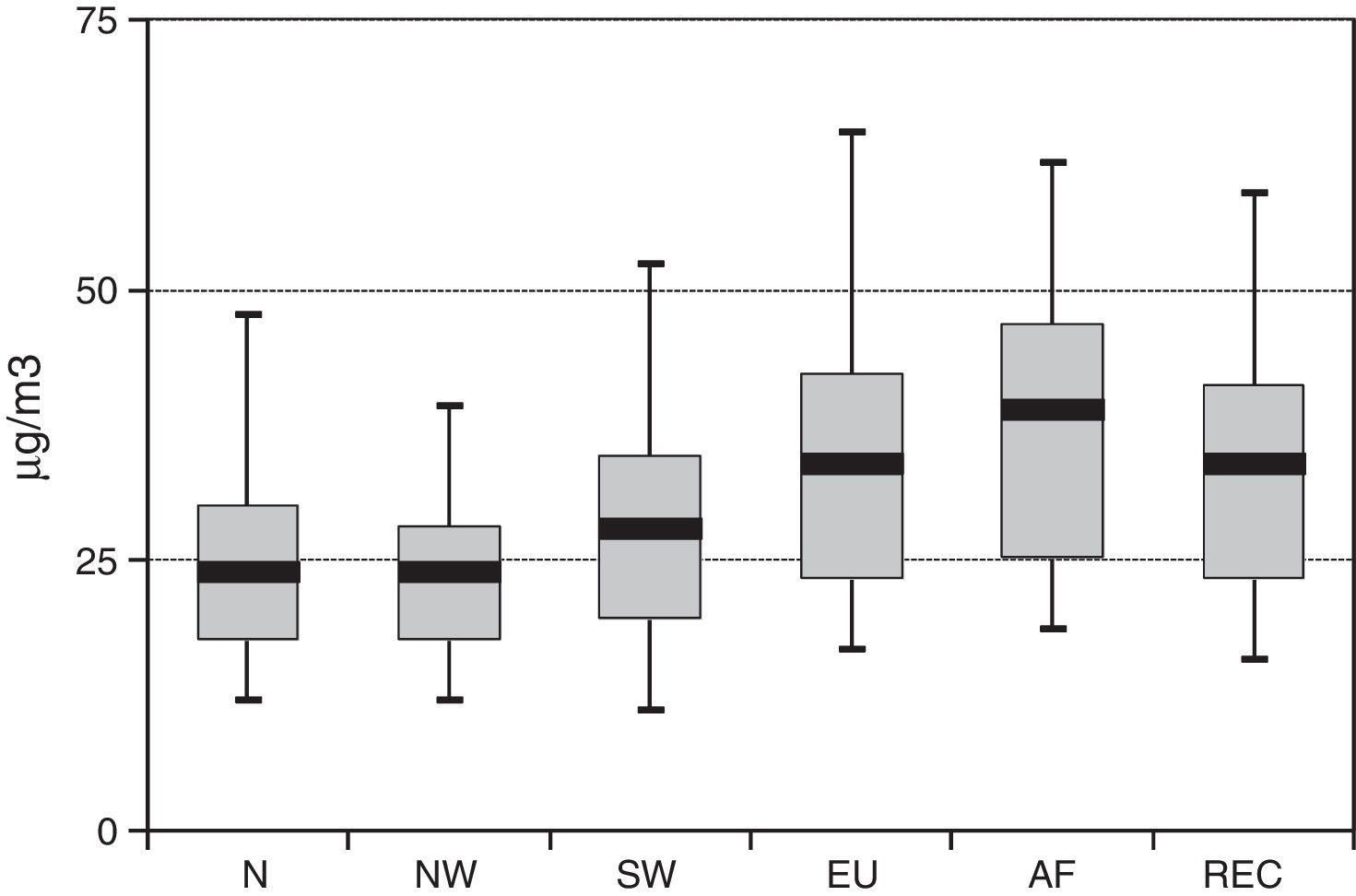
When N and EU trajectories prevail on the synoptic scale, no association is found between PM10 levels and COPD emergencies, either globally or in older adults.
However, when AFR trajectories prevail on the synoptic scale, the effect of PM10 on COPD decompensation increases significantly, insofar as hospital visits increased by 4.58% for every 10μg/m3 increase in PM10 levels (P=.00006).
Similarly, emergency visits by adults aged over 75 years increased by 6.11% (P=.0002) for every 10μg/m3 increase in PM10 levels when the trajectory was AFR, and by 6.13% under recirculation weather conditions (P=.00006).
An association between PM10 and emergency visits is also found with NW and SW air mass trajectories, although the effect is milder (Table 1).
Increased Risk of Emergency Visits for COPD According PM10 Levels and Atmospheric Circulation Patterns, With a 95% Confidence Interval.
| Total Population | Population Aged 75 and Over | |||||
|---|---|---|---|---|---|---|
| Risk Percentage Increase | Confidence Interval | P-Value | Risk Percentage Increase | Confidence Interval | P-Value | |
| Particulate matter (PM10) | ||||||
| Atmospheric circulation | ||||||
| Global | 3.34 | 1.71–4.99 | .000052 | 3.75 | 1.41–6.14 | .001538 |
| N | – | – | – | – | – | – |
| NW | 2.45 | 0.62–4.32 | .008378 | 4.29 | 1.63–7.02 | .001420 |
| SW | 2.96 | 1.31–4.64 | .000393 | 5.19 | 2.81–7.63 | .000015 |
| EU | – | – | – | – | – | – |
| AFR | 4.58 | 2.32–6.90 | .000061 | 6.11 | 2.84–9.49 | .000203 |
| RECIRC | 3.49 | 1.34–5.69 | .001345 | 6.13 | 3.08–9.27 | .000064 |
The most important results of the this study are: (1) there is a direct association between PM10 levels and emergency visits for COPD, and the effect of air pollutants is greater in patients aged over 74 years; (2) on days in which oceanic air masses predominate (SW, NW, N), aerosol levels are lower than when continental conditions (RECIRC, AFR, EU) prevail; (3) when PM10 levels are derived from Northern African air masses crossing the peninsula, and during slow-moving and recirculation (RECIRC) weather conditions, the number of COPD emergencies increases.
Some authors claim that COPD is more closely linked with air pollution than any other respiratory disease, and that the incidence and severity of this condition has increased since industrialization.22
Schikowski et al. found a decrease in forced expiratory volume in one second and an increased risk of COPD associated with PM10 levels caused by urban traffic. The same authors showed that long-term exposure to an environment with high particulate levels (7μg/m3 higher than normal) was associated with a 33% increase in the risk of COPD.23 It is interesting to note that while an increased level of air pollution is associated with negative health effects, a reduction in environmental PM10 levels can reverse some of these effects and improve pulmonary function.24
The first finding reported in this study in the city of Santander is consistent with those reported in other countries.25 However, in this study we have shown for the first time that prevention measures cannot be based exclusively on the PM10 concentrations measured in a certain area, but that the origin and the trajectory of the aerosols making up those concentrations are also of fundamental interest.
The composition of the particles varies continuously and significantly from one geographical area to another. Anthropogenic particles typically contain harmful chemical compounds that are usually smaller in diameter than natural aerosols, enabling them to penetrate the body's defences and reach the terminal bronchioles and alveoli. Because of their smaller size, they can remain suspended in the air for longer periods, and are more easily carried be the wind. This could explain why PM10, unlike NO2, is not such a significant problem in Central Europe, whereas PM10 levels are much higher in the Mediterranean region of Europe due to a combination of human (traffic) and natural (Sahara dust) input.
Interestingly, the N and EU trajectories, which travel through Europe, are not associated with an increase in PM10-related emergency visits for COPD. In theory, the anthropogenic input in these trajectories is much greater than that of AFR (North Africa), which is mostly composed of natural particles (Saharan dust). However, if we consider the possible origin of the pollutants on a mesoscale (which is a smaller weather system than the synoptic meteorological scale, whose horizontal dimensions range from about 9 to several hundred kilometres), the main industrial source is located to the south-east of Santander, in the Camargo area. Here, the natural particulates carried by the AFR and RECIRC systems probably combine with anthropogenic input from the southern end of the bay, which could explain why the number of PM10-based emergency visits for COPD increases when these conditions prevail. Arruti et al. analyzed the content of local industry-derived metals in PM10, and showed that manganese and lead (emitted from factories located to the south of Santander and known to be harmful to the respiratory system) were the major contributors.26,27
Our study has some limitations that should be addressed in future research. First, the lack of a standard system for classifying emergencies in our hospital means that errors could have been made when including patients in our study based purely on the attending physician's diagnostic impression (some eligible patient might have been excluded, or some might have been included in the COPD group when they were in fact seen for another disease). Secondly, although we analyzed 8-year daily data, we do not have specific information for each patient, and considering the multifactorial nature of COPD, the inclusion of more risk variables would have strengthened our results. Furthermore, since other studies have found an association between COPD and several pollutants such as NO2 or SO2, and our study only found a statistically significant relation with PM10, we believe that it is important to emphasize that this may be due to the low levels of these pollutants in the study region. Cantabria is a province with little industrial activity and small areas of intense traffic, and levels of atmospheric pollutants were below the threshold recommended by the WHO nearly every day over the study period. Finally, we believe it would have been interesting to include smaller diameter particles (PM2.5) in the analysis. However, these could not be included because PM2.5 monitoring did not start in Cantabria until 2009, and no continuous data are available.
To conclude, we would draw attention to a recently published study that highlights the importance of taking into consideration atmospheric PM10 levels in the control and follow-up of COPD patients living in urban areas.28 Nowadays, air pollution levels can be forecast in many cities using simulation-based, highly detailed air quality modelling systems, such as CALIOPE,29 which can predict meteorological conditions and the distribution of atmospheric pollutants. These tools can form the basis of early warning systems that will allow healthcare services to set aside the resources needed to meet the expected demand. Our findings also raise the need for information on the composition of particulate matter. Back-trajectories are a useful tool in this respect, although they are seldom used in the field of operational forecasting.
Conflict of InterestThe authors declare they have no conflict of interest.
We thank Dr. Rojo, admitting physician at the Hospital Universitario Marqués de Valdecilla, for his help in collecting emergency care data, and Aurora Ortega, Head of the User Relationship Management department of the AEMET Cantabria office, for providing us with meteorological variables and explaining their characteristics and collection method.
Please cite this article as: Santurtún A, Rasilla DF, Riancho L, Zarrabeitia MT. Análisis de la relación entre la enfermedad pulmonar obstructiva crónica y los contaminantes atmosféricos atendiendo al origen y trayectoria de las masas de aire en el Norte de España. Arch Bronconeumol. 2017;53:616–621.







