
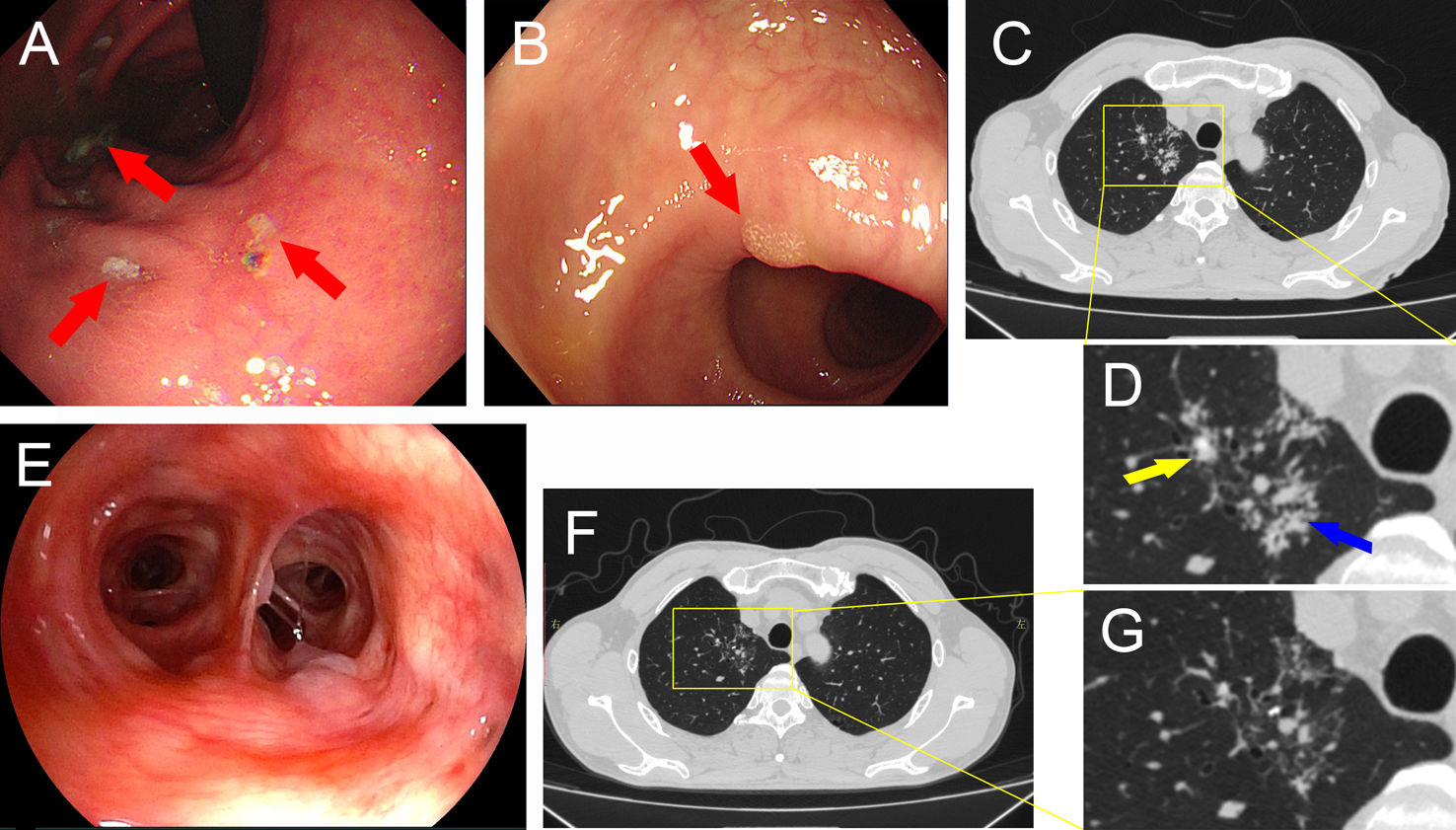
A 59-year-old male had been experiencing epigastric discomfort for nearly five years and a recent paroxysmal cough. Gastroscopy revealed the presence of multiple ulcers at the gastric angle (Fig. 1A) and colonoscopy identified a polyp in the sigmoid colon (Fig. 1B). The chest CT scan revealed pulmonary nodules and patchy opacities in the apical segment of the right upper lobe (Fig. 1C and D). The blood routine examinations were within normal limits. Fiberoptic bronchoscopy revealed no notable abnormalities (Fig. 1E). T-spot testing and bronchial brushing cytology were negative. Microbiological cultures of sputum, blood, stool and bronchoalveolar lavage fluid (BALF) did not reveal any significant pathogens. Fortunately, Tropheryma whipplei was successfully identified in the BALF using metagenomic next-generation sequencing. Subsequently, the patient was initiated on a standardized treatment regimen of oral 100mg doxycycline twice daily for a duration of 12 weeks. Outpatient follow-up revealed resolution of the paroxysmal cough and epigastric discomfort. The chest CT scan performed three months later demonstrated a reduction in pulmonary nodules and patchy opacities (Fig. 1F and G).
. Colonoscopy showed a polyp in the sigmoid colon (B). Chest CT images revealed pulmonary nodules (yellow arrow) and patchy opacities (blue arrow) in the apical segment of the right upper lobe (C and D). Fiberoptic bronchoscopy with no notable abnormalities (E). Chest CT 3 months after treatment with doxycycline (F and G).")
Gastroscopy revealed the presence of multiple ulcers at the gastric angle (A). Colonoscopy showed a polyp in the sigmoid colon (B). Chest CT images revealed pulmonary nodules (yellow arrow) and patchy opacities (blue arrow) in the apical segment of the right upper lobe (C and D). Fiberoptic bronchoscopy with no notable abnormalities (E). Chest CT 3 months after treatment with doxycycline (F and G).
T. whipplei is widely distributed in the environment and the clinical presentation of the disease is highly variable with multiple organ systems affected.1,2 Here, we present a case of pulmonary infection caused by T. whipplei, without typical symptoms such as diarrhea or joint manifestations. Treatment with oral doxycycline proved to be effective. It is important to consider the possibility of T. whipplei infection in patients presenting with pulmonary nodules and patchy infiltration, given the association between T. whipplei and these radiographic findings.
FundingThis work was supported by the Youth Science and Technology Project of Suzhou (KJXW2021079); the Scientific Research Project of Suzhou Ninth People's Hospital (YK202106).
Conflict of InterestsThe authors state that they have no conflict of interests.







