



We report the case of a 69-year-old man, former smoker, who attended the emergency department with constitutional symptoms and pain in the right shoulder. Chest radiograph (Fig. 1A and B) revealed a mass in the right upper lobe. His symptoms were controlled and he was referred to the respiratory medicine department, where positron emission tomography and chest computed tomography (CT) were performed, showing destruction of the ribs by the mass with incipient signs of subcutaneous emphysema. A few days after the biopsy (epidermoid carcinoma), he presented in our hospital with significant clinical deterioration. Examination revealed cervicofacial swelling, thoracocervical crackles, and hypophonesis in right fields, with tachypnea and arterial oxygen saturation of 93%. Urgent CT was performed (Fig. 1C), showing pneumomediastinum and massive subcutaneous emphysema. The patient was admitted to the oncology department, where 2 subcutaneous Penrose® drainage tubes were inserted, producing clinical and radiological improvement.
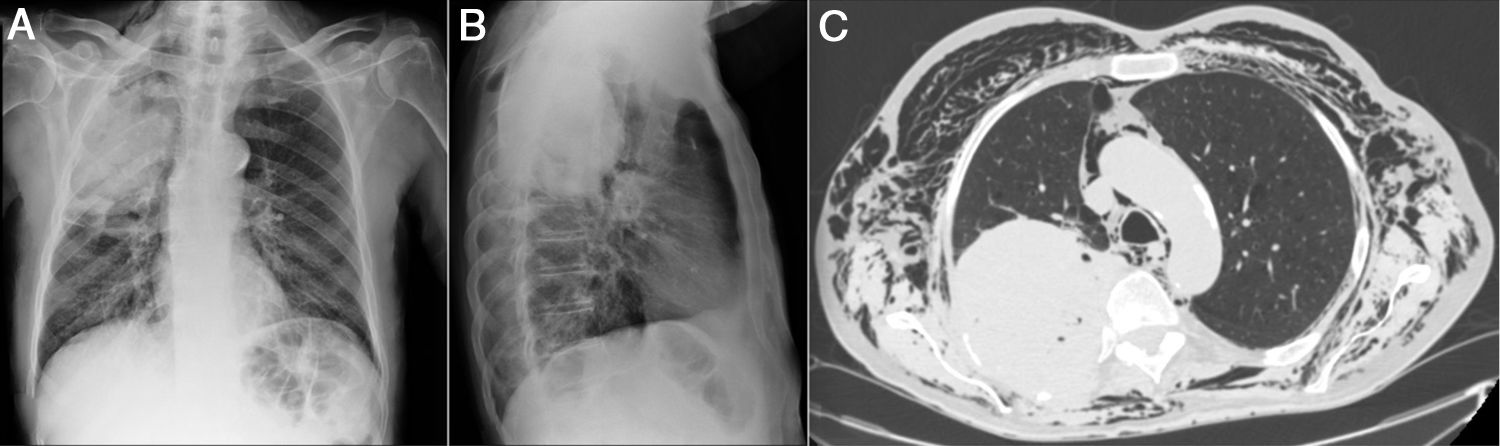
(A and B) Plain chest X-ray in PA and lateral projections. Voluminous mass in right upper lobe, and minor cervical subcutaneous emphysema. (C) Chest CT (axial slice, mediastinum window). Resorption of posterior costal arches at the site of the mass, pneumomediastinum and massive subcutaneous emphysema.
Pneumomediastinum with subcutaneous emphysema due to lung cancer is a rare entity attributed to tracheomediastinal fistula.1 In our case, rib resorption had caused a subcutaneous bronchopleural fistula. Treatment of uncomplicated emphysema is conservative (oxygen therapy, analgesia, antibiotics), but in case of hemodynamic or respiratory involvement, skin incisions and drainage tubes can be used to release air.2
Please cite this article as: Láinez-Ramos-Bossini AJ, Pérez-García MC, Rueda-Cáceres MT. Neumomediastino y enfisema subcutáneo masivo secundarios a neoplasia pulmonar. Arch Bronconeumol. 2020;56:4560.







