
Specialized care outpatient clinics tend to be inundated by high numbers of patients referred from primary care centers (PCC).1 This overload seriously undermines the management of waiting lists and delays the evaluation of patients with severe diseases.2,3 Long waiting lists are the result of a shortage of human resources, work systems, and interdependency between PCC and specialized care facilities. In the Canary Islands, these problems are compounded by geographical obstacles and the remote location of communities. Tenerife has a surface area of 2034.38km2 and an estimated population of 906,854 inhabitants, making it the most heavily populated island in Spain. Most of the population is concentrated in 3 areas: Santa Cruz de Tenerife, San Cristobal de la Laguna and the municipalities of Arona and Adeje. The latter 2, located in the south of the island, have a resident population of 200,000 inhabitants, and the nearest tertiary hospital is at least 80km away.
The disperse population in the south of the island and their ensuing transport difficulties led to the implementation in June 2012 of the Respiratory Virtual Clinic, the aim of which was to manage and prioritize pulmonology referrals from PCC. The Respiratory Virtual Clinic takes place 2 days a week, and up to 15 cases are discussed in each session. The consultant pulmonologist prioritizes cases by examining the data provided online by the PCC (clinical history, physical examination, complementary tests) and performs a triage, by either indicating to the treating physician the procedure to follow, or by personally evaluating the patient. In the latter case, the tests required for the first appointment are performed on the same day in the outpatient clinic (chest X-ray, spirometry or blood gases), and the patient is referred directly to the right clinic: either the general pulmonology clinic held 4 days a week or else the dedicated COPD clinic, which takes place once a week. Patients already monitored in the pulmonology clinic whose respiratory disease worsens can immediately access either of the 2 clinics without the need for a referral from the PCC.
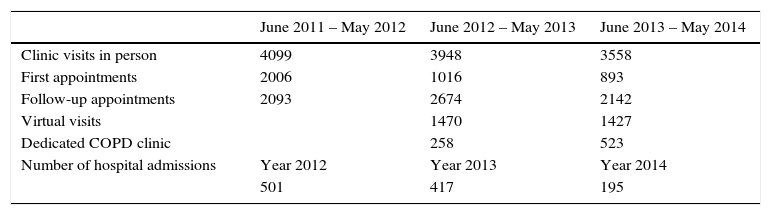
In less than 3 years, this formula has reduced the overall number of PCC consultations by 14%, and the number of first appointments by 56%. The reduction in workload meant that chronic patients can be more closely monitored, leading to a 61% reduction in the number of hospital admissions to the pulmonology department, while follow-up appointments rose by 15% (Table 1).
Number of Visits and Patients Seen in the Pulmonology Department.
| June 2011 – May 2012 | June 2012 – May 2013 | June 2013 – May 2014 | |
|---|---|---|---|
| Clinic visits in person | 4099 | 3948 | 3558 |
| First appointments | 2006 | 1016 | 893 |
| Follow-up appointments | 2093 | 2674 | 2142 |
| Virtual visits | 1470 | 1427 | |
| Dedicated COPD clinic | 258 | 523 | |
| Number of hospital admissions | Year 2012 | Year 2013 | Year 2014 |
| 501 | 417 | 195 |
Finally, the Respiratory Virtual Clinic increased the number of consultations that could be resolved by the PCC by 19%, underscoring the efficiency of this type of management.
Please cite this article as: Figueira JM, Hernández Gracia MC, Batista Martín JJ. Una nueva gestión ambulatoria basada en la consulta virtual de neumología. Una medida efectiva en tiempos de «austeridad». Arch Bronconeumol. 2016;52:279–280.







