



We report the case of a 73-year-old man, active smoker with no other significant medical history, who presented with central chest discomfort and weight loss. The first chest X-ray revealed a retrocardiac opacity with well-defined margins, containing an air-fluid level, initially suggesting a diagnosis of paraesophageal hiatal hernia, since part of the stomach was visualized in the left subphrenic region (Fig. 1A and B). Three weeks later, the patient consulted due to a self-limiting episode of hemoptysis; chest CT at that time showed an extensively cavitated pulmonary mass (Fig. 1C and D) with mediastinal infiltration. Squamous cell lung cancer was confirmed by fiberoptic bronchoscopy.
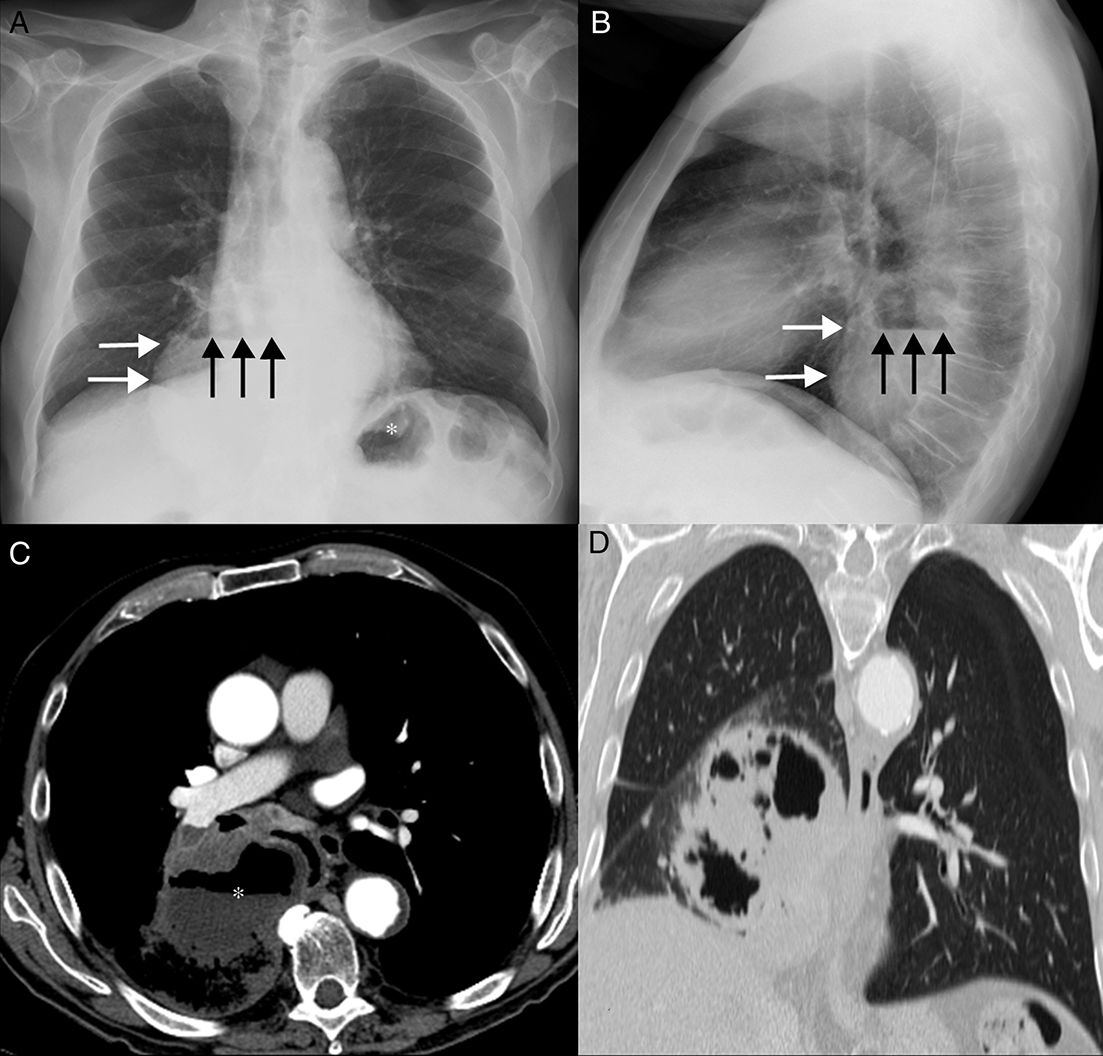
(A) Posteroanterior chest X-ray showing opacity in the right hemithorax (white arrows) containing an air-fluid level (black arrows). Note the gastric fundus (asterisk) protruding into the left subphrenic region. (B) Lateral chest X-ray confirming the retrocardiac location of the opacity (white arrows) with the air-fluid level (black arrows). (C) Axial CT image showing an extensively necrotic, cavitary mass (asterisk) in the paramediastinal region of the right lower lobe. Note the presence of an air-fluid level in the cavitated area. (D) Coronal CT image (pulmonary parenchymal window) confirming intrapulmonary lesion and preserved hemidiaphragms.
Paraesophageal hiatal hernias occur when the gastric fundus protrudes up through the esophageal hiatus, while the gastroesophageal junction remains in a normal subphrenic position. Cases have been described in the literature in which hiatal hernia mimics pulmonary or mediastinal masses on imaging tests.1,2 However, we have found no descriptions of cases such as ours in which an extensively cavitated lung cancer radiologically mimicked an intrathoracic hiatal hernia.
Please cite this article as: Sarasúa LG, González-García A, García Gómez-Muriel I. Carcinoma broncogénico extensamente cavitado simulando una hernia de hiato paraesofágica. Arch Bronconeumol. 2018;54:427.







