
To assess whether changes in pleural fluid (PF) biochemistries between two consecutive thoracenteses enable clinicians to predict malignant or benign pleural effusions (PE).
MethodsRetrospective study of patients with lymphocytic exudates and negative PF cytology, who underwent a second thoracentesis in our center in the last 15 years in whom a final diagnosis was reached (derivation sample). Absolute (Δa) and percentage differences (Δp) in PF biochemistries which predicted a malignant or benign PE in the derivation sample were evaluated in an independent population (validation sample).
ResultsThe derivation sample included 214 PE patients (70 malignant and 144 benign PE). Δp lactate dehydrogenase (LDH)>0%, Δp neutrophils>−10% (any increase or less than 10% decrease) and Δa protein <0.1g/dL (any increase or less than 0.1g/dL decrease) between the second and the first thoracentesis had an odds ratio of 6.4, 3.9 and 2.1, respectively, to discriminate malignant from benign PE. The presence of the three conditions together had a positive likelihood ratio of 5.6, whereas the absence of any of the three parameters had a likelihood ratio of 0.04 for predicting malignancy. These results were reproduced in the validation sample.
ConclusionAn increase in LDH and neutrophils along with a decrease in protein in a second thoracentesis increase the probability of malignant PE, while the opposite reduces it significantly.
Evaluar si los cambios en los parámetros bioquímicos del líquido pleural (LP) entre 2 toracocentesis sucesivas permiten predecir derrames pleurales (DP) malignos o benignos.
MétodosEstudio retrospectivo de los pacientes con exudado linfocitario y citología negativa para malignidad que se sometieron a una segunda toracocentesis en nuestro centro durante los últimos 15 años (muestra de derivación), y en los que se alcanzó un diagnóstico final. Las diferencias absolutas (Δa) o porcentuales (Δp) de diferentes parámetros bioquímicos del LP capaces de predecir la naturaleza maligna o benigna del DP en la muestra de derivación se evaluaron en una población independiente.
ResultadosSe incluyeron 214 pacientes con DP (70 malignos y 144 benignos) en la muestra de derivación. Las Δp LDH (lactato deshidrogenasa) > 0%, Δp neutrófilos > –10% (cualquier aumento o bien un descenso inferior al 10%), y Δa proteínas < 0,1g/dL (cualquier descenso o bien un aumento inferior a 0,1g/dL) entre la segunda y primera toracocentesis mostraron unas odds ratio de 6,4, 3,9 y 2,1 para discriminar DP maligno de benigno, respectivamente. La presencia de las 3 condiciones conjuntamente se asoció con una likelihood ratio positiva de 5,6, mientras que la ausencia de cualquiera ellas se asoció con una likelihood ratio negativa de 0,04 para predecir malignidad. Los resultados se reprodujeron en la población de validación.
ConclusiónEl aumento de LDH y neutrófilos, junto con el descenso de proteínas en una segunda toracocentesis, aumenta la probabilidad de que el origen del DP sea neoplásico, mientras que lo contrario la reduce significativamente.
Pleural effusion (PE) is a common medical problem that has more than 60 recognized causes.1 Cancer is the most common reason for PE studied by thoracentesis, accounting for around 30% of cases.2 The diagnosis of malignant PE is definitive when cancer cells are detected in a cytological study of the pleural fluid (PF). However, only 51% of tests are positive in the first analysis.2 Analysis of new PF samples can increase the diagnostic yield to around 60%, so the percentage of false negatives on cytology is significant.3 Moreover, only 34% of malignant PEs are associated with a history of cancer that could orient the clinician toward the potentially cancerous nature of the specimen.4
The biochemical parameters of PF offer more immediate information on this type of specimen. Malignant PE is typically an exudate with a predominance of lymphocytes.5 A second diagnostic thoracentesis is often performed while awaiting results from the first cell block or when the cytology results from the first sample are negative. If two cytological studies of PF that include a cytology smear and a cell block are negative, yet malignancy is suspected, a diagnostic thoracoscopy is recommended.5 However, this technique is invasive, so it should be reserved for patients who might benefit from the procedure.6
Some experts suggest that the serial measurement of lactate dehydrogenase (LDH) in PF may help guide diagnosis in patients with PE of uncertain etiology, since this enzyme is a reliable indicator of the degree of pleural inflammation.7 A progressive increase in LDH levels observed on a repeat thoracentesis indicates increased inflammation in the pleural space, and the search for an accurate diagnosis should continue. However, if LDH levels fall, the process is probably resolving, and invasive diagnostic procedures can be avoided. This theory, however, is based purely on expert opinion, and has not been corroborated in any study.
The aim of this study was to evaluate and validate changes in LDH and other biochemical variables in PF in successive thoracentesis as predictors of malignant or benign PE. This may help to select patients who would require more intensive investigation for a definitive diagnosis with the use of procedures such as thoracoscopy.
Materials and MethodsPatient SelectionThis was a retrospective study that included all consecutive patients with PE seen in the Hospital Universitario Arnau de Vilanova de Lleida between January 2001 and December 2016 who met the following criteria (derivation sample): (a) at least two diagnostic thoracenteses with available biochemical data on PF (if three or more thoracenteses were performed, only the first two were considered); (b) PF in the first thoracentesis was an exudate (according to Light's criteria8) with >50% lymphocytes in the leukocyte count and a negative cytology for malignancy; and (c) a definitive diagnosis for PE etiology or else PE determined to be idiopathic (see definition below). The Hospital Universitario Arnau de Vilanova de Lleida is a 440-bed reference hospital with a catchment population of 450000 inhabitants, and carries out around 400 diagnostic thoracenteses per year.
Patients were divided into two groups according to the final diagnosis: malignant PE and benign PE. The benign PE group was then subdivided into idiopathic and other etiologies. Absolute and relative changes in the PF biochemical variables between two successive thoracentesis considered significant in the derivation sample were validated in a population with the same inclusion criteria, seen in the Hospital de Mendaro between January 1995 and August 2015 (validation sample). Hospital de Mendaro is a 125-bed county hospital with a catchment population of 80000, and performs 50 diagnostic thoracenteses every year.
The following variables were recorded: demographic data (sex and age); date of both thoracenteses; protein and LDH serum concentrations; and red blood cell and white blood cell counts, neutrophil and lymphocyte percentages, glucose, LDH, proteins, adenosine deaminase (ADA), pH, and C-reactive protein (CRP) in PF. The local ethics committee approved the study protocol (CEIC-1592).
Diagnostic CriteriaPE was defined as malignant if malignant cells were found in PF or pleural biopsy. PE due to heart failure was diagnosed from the clinical history, physical examination, chest X-ray, electrocardiogram, echocardiogram (if available), and good response to diuretics. Confirmation of a diagnosis of pleural tuberculosis required tuberculosis bacillus to be isolated from sputum samples, PF or pleural biopsy, or granulomas observed in the latter. Pleural tuberculosis was considered likely in patients with lymphocytic exudate and ADA≥35U/L in PF, whose PE resolved with antituberculosis treatment. Parapneumonic PEs were those associated with pneumonia, bronchiectasis, or pulmonary abscess. Finally, PE was classified as idiopathic when it resolved with no specific treatment and its etiology could not be determined despite an in-depth study that included PF analysis (biochemistry, cytology), chest and abdominal computed tomography (CT), and, in selected cases, pleural biopsy. Other diagnoses were established according to widely accepted clinical criteria.2 All patients with benign pleural diseases were followed up clinically until complete resolution of the PE, which, in the case of idiopathic PE, was at least a year.
Pleural Fluid AnalysisPF was collected from the derivation population in 5mL heparinized tubes, and biochemical analysis was performed immediately after thoracentesis using an automatic analyzer, according to standard spectrophotometric methods (Hitachi 717 and 911 or Hitachi Modular PE, Roche Diagnostics, Mannheim, Germany) until August 2013, and subsequently with an AU5800 Beckman Coulte analyzer (Brea, CA, USA). The pH was analyzed using an arterial blood gases machine and ADA was determined with automated kinetic methods. Until February 2012, the PF cell count was performed manually in a Thoma counting chamber, and subsequently with automatic counters (Sysmex XN-2000 and Sysmex XN-350; Roche Diagnostics, Mannheim, Germany).
In the validation population, PF was collected in 15mL Falcon tubes containing 1mL of heparin. Biochemical variables were analyzed with a Cobas 6000 autoanalyzer (Roche Diagnostics, Mannheim, Germany). The pH was measured using an arterial blood gas analyzer, and ADA was determined with automated kinetic methods. Until December 2016, PF cell counts were determined in a Neubauer Improved counting chamber, and subsequently in an automated system (Sysmex SN-2000 and Sysmex XN-350, Roche Diagnostics, Mannheim, Germany).
Statistical AnalysisCategorical variables were expressed as absolute numbers (percentages) and continuous variables as medians (25th and 75th percentiles). Benign and malignant PEs were compared with Fisher's exact test and the Mann–Whitney test, respectively. Variables associated with malignant, idiopathic and other benign PEs were compared with the Fisher's exact and Kruskal–Wallis tests, as appropriate.
The Wilcoxon test was used to compare biochemical parameters between the first and the second thoracentesis. For variables that showed significant differences between the two thoracenteses in any of the etiological groups (malignant, idiopathic, or other benign), we calculated both absolute differences (Δa=value of the variable in the second thoracentesis minus the value of the variable in the first thoracentesis) and percentage differences (Δp=value of the variable in the second thoracentesis minus the value of the variable in the first thoracentesis, divided by the value of the variable in the first thoracentesis).
An area under the curve (AUC) analysis of diagnostic efficacy was used to select the best cut-off point for continuous variables (Δa and Δp) that could predict malignant or benign PE. A multivariate logistic regression analysis, which included the dichotomous Δa or Δp of the biochemical variables that were significant in the bivariate analysis, was used to calculate the odds ratio (OR) of the Δa and Δp to identify the benign or malignant nature of the PE. Operational characteristics of the Δa and Δp were calculated using a 2×2 contingency table (sensitivity, specificity, positive and negative likelihood ratio [LR]) for both the derivation population and the validation population. Statistical significance was set at P≤.05. All statistical tests were performed using version 24.0 of the SPSS statistical package (Chicago, IL, USA).
ResultsCharacteristics of the Study PopulationThe derivation population included 214 patients, representing 12% of all subjects with lymphocytic exudate evaluated in our hospital during the study period. Seventy (33%) had malignant PE, and the most common cancers were lung (19, 27%), breast (14, 20%) and mesothelioma (10, 14%). The final diagnosis of malignancy was obtained by subsequent cytological studies of PF (41 patients), cellular phenotyping of PF by flow cytometry (three patients), CT-guided pleural biopsy (11 patients), ultrasound-guided pleural biopsy (six patients), and thoracoscopic pleural biopsy (nine patients). Of the 144 benign PEs, 44 (31%) were classified as idiopathic. Of the latter, pleural biopsy was performed in only 11 cases (25%); in 28 (64%) the biopsy was considered a risk procedure (and was not performed), due to the presence of a PE that occupied one third or less of the hemithorax.
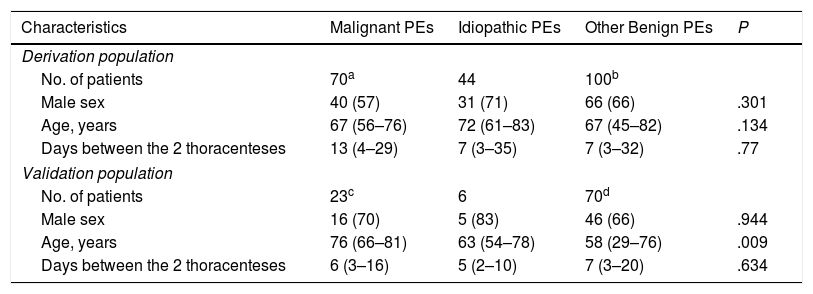
The validation sample included 99 patients (i.e., 15% of the lymphocytic exudates diagnosed in the corresponding hospital during the study period). Of these, 23 were diagnosed as malignant PE in subsequent cytology studies (six patients), cellular immunophenotyping of the PF by flow cytometry (three patients), and thoracoscopic biopsy (14 patients). Table 1 shows the characteristics of the derivation and validation populations. No differences were observed in the interval (days) between thoracenteses in the different etiological groups. Nor were differences observed between the overall derivation and the validation populations (medians of 8 [3–31] vs 6 [3–16] days, P=.132), or etiologic groups: malignant PE (medians of 13 [4–29] vs 6 [3–16] days, P=.147), and benign PEs (medians of 7 [3–33] vs 6 [3–18] days; P=.389).
Characteristics of the Study Population.
| Characteristics | Malignant PEs | Idiopathic PEs | Other Benign PEs | P |
|---|---|---|---|---|
| Derivation population | ||||
| No. of patients | 70a | 44 | 100b | |
| Male sex | 40 (57) | 31 (71) | 66 (66) | .301 |
| Age, years | 67 (56–76) | 72 (61–83) | 67 (45–82) | .134 |
| Days between the 2 thoracenteses | 13 (4–29) | 7 (3–35) | 7 (3–32) | .77 |
| Validation population | ||||
| No. of patients | 23c | 6 | 70d | |
| Male sex | 16 (70) | 5 (83) | 46 (66) | .944 |
| Age, years | 76 (66–81) | 63 (54–78) | 58 (29–76) | .009 |
| Days between the 2 thoracenteses | 6 (3–16) | 5 (2–10) | 7 (3–20) | .634 |
Variables are expressed as n (%) or median (25–75 percentile).
PE: pleural effusion.
Lung cancer, 19; breast, 14; mesothelioma, 10; lymphoma, 7; unknown origin, 4; ovarian, 4; pancreatic, 3; gastric, 2; colon, 2; endometrium, 2; kidney, 1; prostate, 1; hepatocellular carcinoma, 1.
Tuberculosis, 33 (19 probable and 14 confirmed); heart failure, 24; pericarditis, 14; post-surgical, 9; parapneumonic, 7; connective tissue disease, 4; secondary to liver abscess, 2; acute pancreatitis, 2; uremia, 2; post-traumatic, 1; iatrogenic chylothorax, 1; atelectasis, 1.
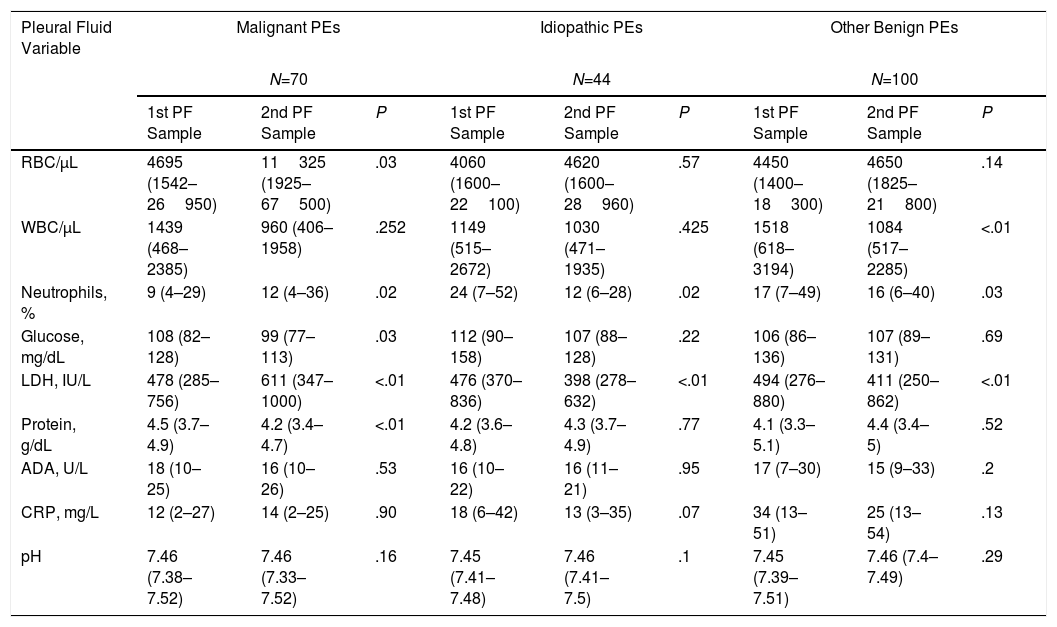
As Table 2 shows, the percentage of neutrophils and LDH levels in PF fell in the second thoracentesis compared to the first in the subgroup of idiopathic PEs (12% vs 24%, P=.02; and 398U/L vs 476U/L, P<.01) and remaining benign PEs (16% vs 17%, P=.03; and 411U/L vs 494U/L, P<.01), but increased in the malignant PE group (12% vs 9%, P=.02; and 611U/L vs 478U/L, P<.01). Increased red blood cells and lower glucose and protein levels in the second PF sample compared to the first were observed only in the malignant PE group (11325/μL vs 4695/μL, P=.03; 99mg/dL vs 108mg/dL, P=.03; and 4.2g/dL vs 4.5g/dL, P<.01, respectively). In the group of other benign PEs, reduced leukocytes were also observed in the second thoracentesis (1084/μL vs 1518/μL, P<.01). Other biochemical variables (ADA, pH, and PCR) showed no differences between the two thoracenteses, so these parameters were ruled out as possible predictors of malignant PE.
Comparison of Pleural Fluid Variables Between 2 Consecutive Thoracenteses (Derivation Population).
| Pleural Fluid Variable | Malignant PEs | Idiopathic PEs | Other Benign PEs | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N=70 | N=44 | N=100 | |||||||
| 1st PF Sample | 2nd PF Sample | P | 1st PF Sample | 2nd PF Sample | P | 1st PF Sample | 2nd PF Sample | P | |
| RBC/μL | 4695 (1542–26950) | 11325 (1925–67500) | .03 | 4060 (1600–22100) | 4620 (1600–28960) | .57 | 4450 (1400–18300) | 4650 (1825–21800) | .14 |
| WBC/μL | 1439 (468–2385) | 960 (406–1958) | .252 | 1149 (515–2672) | 1030 (471–1935) | .425 | 1518 (618–3194) | 1084 (517–2285) | <.01 |
| Neutrophils, % | 9 (4–29) | 12 (4–36) | .02 | 24 (7–52) | 12 (6–28) | .02 | 17 (7–49) | 16 (6–40) | .03 |
| Glucose, mg/dL | 108 (82–128) | 99 (77–113) | .03 | 112 (90–158) | 107 (88–128) | .22 | 106 (86–136) | 107 (89–131) | .69 |
| LDH, IU/L | 478 (285–756) | 611 (347–1000) | <.01 | 476 (370–836) | 398 (278–632) | <.01 | 494 (276–880) | 411 (250–862) | <.01 |
| Protein, g/dL | 4.5 (3.7–4.9) | 4.2 (3.4–4.7) | <.01 | 4.2 (3.6–4.8) | 4.3 (3.7–4.9) | .77 | 4.1 (3.3–5.1) | 4.4 (3.4–5) | .52 |
| ADA, U/L | 18 (10–25) | 16 (10–26) | .53 | 16 (10–22) | 16 (11–21) | .95 | 17 (7–30) | 15 (9–33) | .2 |
| CRP, mg/L | 12 (2–27) | 14 (2–25) | .90 | 18 (6–42) | 13 (3–35) | .07 | 34 (13–51) | 25 (13–54) | .13 |
| pH | 7.46 (7.38–7.52) | 7.46 (7.33–7.52) | .16 | 7.45 (7.41–7.48) | 7.46 (7.41–7.5) | .1 | 7.45 (7.39–7.51) | 7.46 (7.4–7.49) | .29 |
Variables are expressed as median (25–75 percentile).
ADA: adenosine deaminase; CRP: C-reactive protein; LDH: lactate dehydrogenase; PE: pleural effusion; PF: pleural fluid.
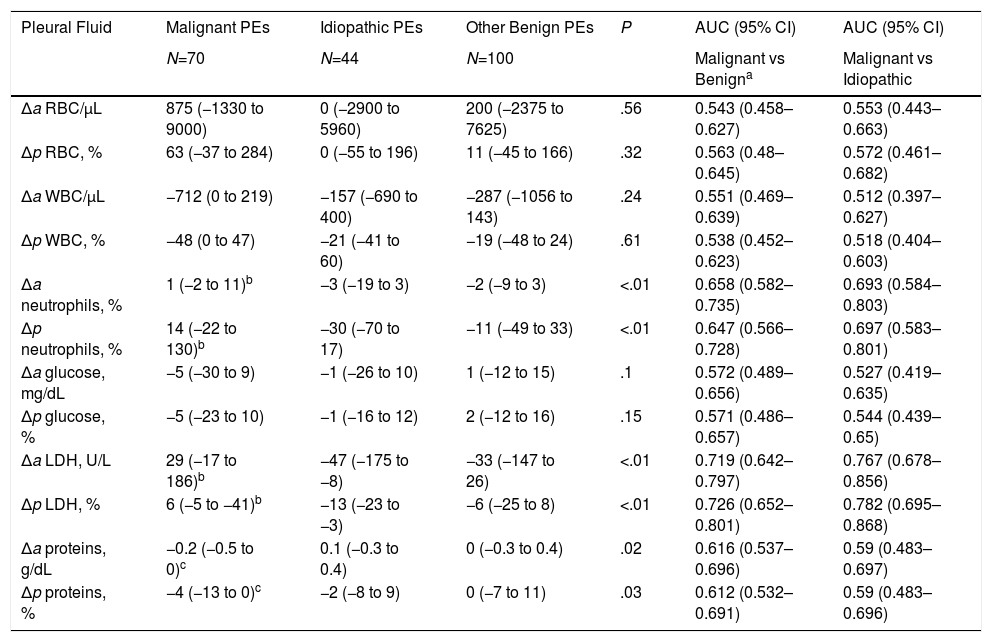
Δa and Δp of the biochemical variables of the PFs that showed significant differences between the two thoracenteses were analyzed (Table 3). Those which best discriminated between a malignant PE and a benign PE (including idiopathic PEs) were: Δp for LDH (AUC 0.73, 95% confidence interval [95% CI]: 0.65–0.8), Δp for neutrophils (AUC 0.65, 95% CI: 0.57–0.73) and Δa for proteins (AUC 0.61, 95% CI: 0.54–0.7).
Medians (25th and 75th Percentiles) of the Absolute and Percentage Differences of Biochemical Variables of Pleural Fluid Between Two Successive Thoracenteses (Derivation Population).
| Pleural Fluid | Malignant PEs | Idiopathic PEs | Other Benign PEs | P | AUC (95% CI) | AUC (95% CI) |
|---|---|---|---|---|---|---|
| N=70 | N=44 | N=100 | Malignant vs Benigna | Malignant vs Idiopathic | ||
| Δa RBC/μL | 875 (−1330 to 9000) | 0 (−2900 to 5960) | 200 (−2375 to 7625) | .56 | 0.543 (0.458–0.627) | 0.553 (0.443–0.663) |
| Δp RBC, % | 63 (−37 to 284) | 0 (−55 to 196) | 11 (−45 to 166) | .32 | 0.563 (0.48–0.645) | 0.572 (0.461–0.682) |
| Δa WBC/μL | −712 (0 to 219) | −157 (−690 to 400) | −287 (−1056 to 143) | .24 | 0.551 (0.469–0.639) | 0.512 (0.397–0.627) |
| Δp WBC, % | −48 (0 to 47) | −21 (−41 to 60) | −19 (−48 to 24) | .61 | 0.538 (0.452–0.623) | 0.518 (0.404–0.603) |
| Δa neutrophils, % | 1 (−2 to 11)b | −3 (−19 to 3) | −2 (−9 to 3) | <.01 | 0.658 (0.582–0.735) | 0.693 (0.584–0.803) |
| Δp neutrophils, % | 14 (−22 to 130)b | −30 (−70 to 17) | −11 (−49 to 33) | <.01 | 0.647 (0.566–0.728) | 0.697 (0.583–0.801) |
| Δa glucose, mg/dL | −5 (−30 to 9) | −1 (−26 to 10) | 1 (−12 to 15) | .1 | 0.572 (0.489–0.656) | 0.527 (0.419–0.635) |
| Δp glucose, % | −5 (−23 to 10) | −1 (−16 to 12) | 2 (−12 to 16) | .15 | 0.571 (0.486–0.657) | 0.544 (0.439–0.65) |
| Δa LDH, U/L | 29 (−17 to 186)b | −47 (−175 to −8) | −33 (−147 to 26) | <.01 | 0.719 (0.642–0.797) | 0.767 (0.678–0.856) |
| Δp LDH, % | 6 (−5 to −41)b | −13 (−23 to −3) | −6 (−25 to 8) | <.01 | 0.726 (0.652–0.801) | 0.782 (0.695–0.868) |
| Δa proteins, g/dL | −0.2 (−0.5 to 0)c | 0.1 (−0.3 to 0.4) | 0 (−0.3 to 0.4) | .02 | 0.616 (0.537–0.696) | 0.59 (0.483–0.697) |
| Δp proteins, % | −4 (−13 to 0)c | −2 (−8 to 9) | 0 (−7 to 11) | .03 | 0.612 (0.532–0.691) | 0.59 (0.483–0.696) |
95% CI: 95% confidence interval; Δa: absolute difference (see definition in text); Δp: percentage difference (see definition in text); AUC: area under the ROC curve; LDH: lactate dehydrogenase; PE: pleural effusion.
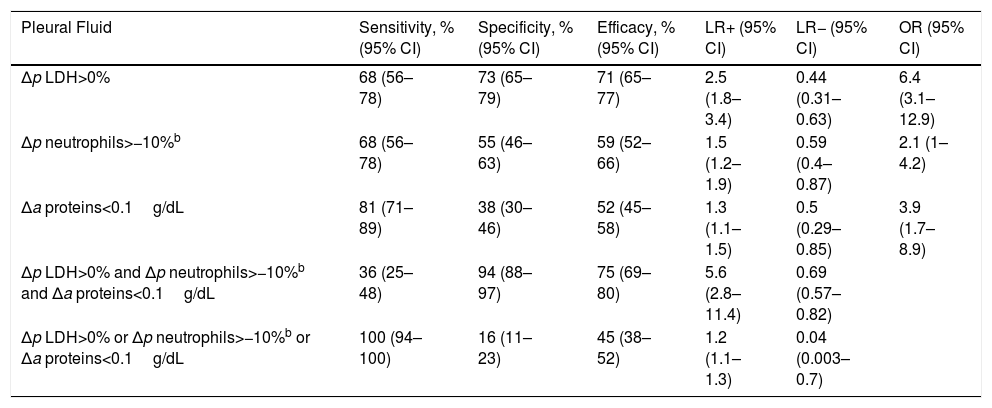
The best cut-off points for these Δa or Δp to discriminate between malignant and benign PE were: Δp LDH>0% (i.e., any increase in LDH in a second thoracentesis), Δp neutrophils>−10% (i.e., any increase or decrease of less than 10%) and Δa proteins<0.1g/dL (i.e., any decrease or an increase of less than 0.1g/dL). In this respect, according to a multivariate model, Δp LDH>0% showed an OR of 6.4 (95% CI: 3.1–12.9); Δp neutrophils>−10% showed an OR of 2.1 (95% CI: 1–4.2) and the Δa for proteins<0.1g/dL showed an OR of 3.9 (95% CI: 1.7–8.9) for identifying malignancy. The same analysis comparing malignant PEs with idiopathic PEs produced the following results: Δp LDH>0%, OR 9 (95% CI: 3.1–26.1); Δp neutrophils>−10% showed an OR of 2.7 (95% CI: 1–7.2) and the Δa for proteins<0.1g/dL showed an OR of 3.8 (95% CI: 1.2–11.8).
Table 4 shows the operational characteristics of the variables selected as predictors of malignant PE vs benign PE. The Δp LDH, Δp neutrophils, and Δa proteins were not useful on an individual basis. However, combinations of the three variables were useful. Thus, a combination of these variables (that is, the combination of Δp LDH>0%, Δp neutrophil −10% and Δa proteins<0.1g/dL) showed a positive LR of 5.6 (95% CI: 2.8–11.4). However, when at least one of the three conditions had to be met, negative LRs were 0.04 (95% CI: 0.003–0.7). Similar results were observed for discriminating between malignant PE and idiopathic PE (Table 5).
Operational Characteristics of Absolute and Percentage Differences in Different Biochemical Parameters of Pleural Fluid for Discriminating Malignant Effusions From Benign Effusionsa (Derivation Population).
| Pleural Fluid | Sensitivity, % (95% CI) | Specificity, % (95% CI) | Efficacy, % (95% CI) | LR+ (95% CI) | LR− (95% CI) | OR (95% CI) |
|---|---|---|---|---|---|---|
| Δp LDH>0% | 68 (56–78) | 73 (65–79) | 71 (65–77) | 2.5 (1.8–3.4) | 0.44 (0.31–0.63) | 6.4 (3.1–12.9) |
| Δp neutrophils>−10%b | 68 (56–78) | 55 (46–63) | 59 (52–66) | 1.5 (1.2–1.9) | 0.59 (0.4–0.87) | 2.1 (1–4.2) |
| Δa proteins<0.1g/dL | 81 (71–89) | 38 (30–46) | 52 (45–58) | 1.3 (1.1–1.5) | 0.5 (0.29–0.85) | 3.9 (1.7–8.9) |
| Δp LDH>0% and Δp neutrophils>−10%b and Δa proteins<0.1g/dL | 36 (25–48) | 94 (88–97) | 75 (69–80) | 5.6 (2.8–11.4) | 0.69 (0.57–0.82) | |
| Δp LDH>0% or Δp neutrophils>−10%b or Δa proteins<0.1g/dL | 100 (94–100) | 16 (11–23) | 45 (38–52) | 1.2 (1.1–1.3) | 0.04 (0.003–0.7) |
95% CI: 95% confidence interval; Δa: absolute difference; Δp: percentage difference; LDH: lactate dehydrogenase; LR: likelihood ratio; OR: odds ratio.
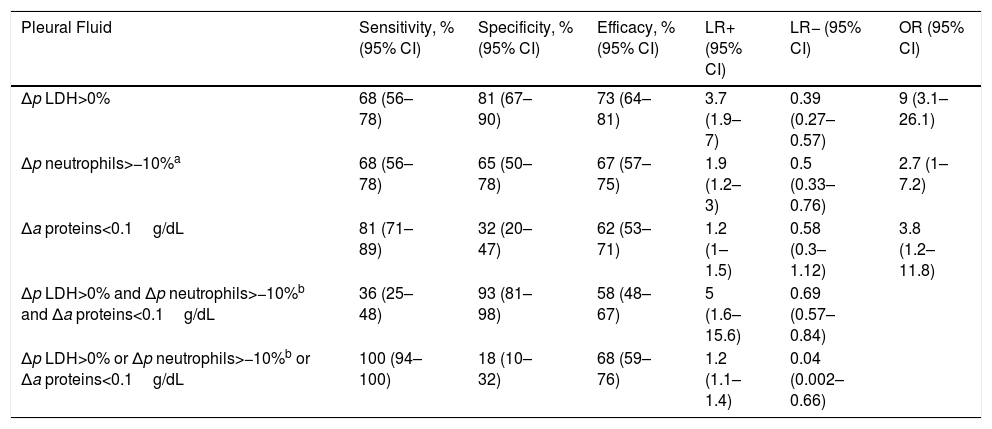
Operational Characteristics of Absolute and Percentage Differences in Different Biochemical Parameters of Pleural Fluid for Discriminating Malignant Effusions From Idiopathic Effusionsa (Derivation Population).
| Pleural Fluid | Sensitivity, % (95% CI) | Specificity, % (95% CI) | Efficacy, % (95% CI) | LR+ (95% CI) | LR− (95% CI) | OR (95% CI) |
|---|---|---|---|---|---|---|
| Δp LDH>0% | 68 (56–78) | 81 (67–90) | 73 (64–81) | 3.7 (1.9–7) | 0.39 (0.27–0.57) | 9 (3.1–26.1) |
| Δp neutrophils>−10%a | 68 (56–78) | 65 (50–78) | 67 (57–75) | 1.9 (1.2–3) | 0.5 (0.33–0.76) | 2.7 (1–7.2) |
| Δa proteins<0.1g/dL | 81 (71–89) | 32 (20–47) | 62 (53–71) | 1.2 (1–1.5) | 0.58 (0.3–1.12) | 3.8 (1.2–11.8) |
| Δp LDH>0% and Δp neutrophils>−10%b and Δa proteins<0.1g/dL | 36 (25–48) | 93 (81–98) | 58 (48–67) | 5 (1.6–15.6) | 0.69 (0.57–0.84) | |
| Δp LDH>0% or Δp neutrophils>−10%b or Δa proteins<0.1g/dL | 100 (94–100) | 18 (10–32) | 68 (59–76) | 1.2 (1.1–1.4) | 0.04 (0.002–0.66) |
95% CI: 95% confidence interval; Δa: absolute difference; Δp: percentage difference; LDH: lactate dehydrogenase; LR: likelihood ratio; OR: odds ratio.
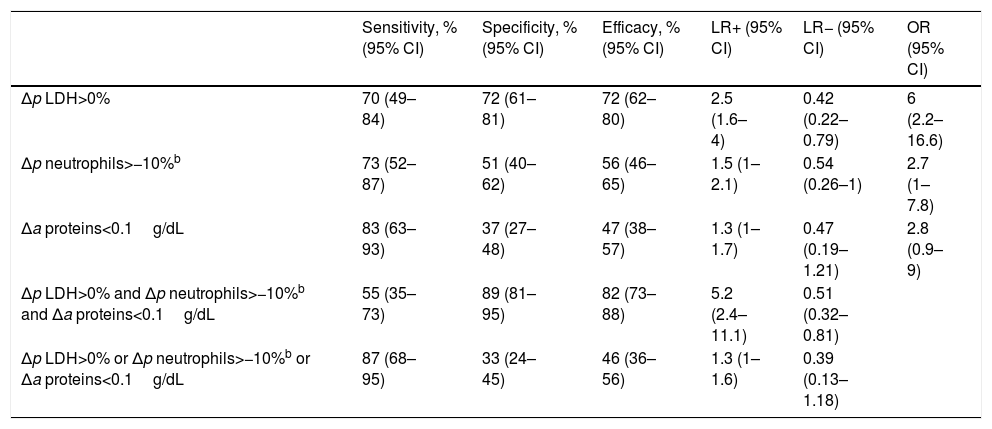
The idiopathic PE group was not considered as independent in the validation population, since it only included six patients. As shown in Table 6, the combination of the three variables that might predict malignant PE, if all three are present, showed a positive LR of 5.2 (95% CI: 2.4–11.1), while if presence of one of the three variables was considered, the negative LR was 0.39 (95% CI: 0.13–1.18); confirming, at least with regard to the combination of all three variables, the results obtained in the derivation population.
Operational Characteristics of Absolute and Percentage Differences in Different Biochemical Parameters of Pleural Fluid for Discriminating Malignant Effusions From Benign Effusionsa (Validation Population).
| Sensitivity, % (95% CI) | Specificity, % (95% CI) | Efficacy, % (95% CI) | LR+ (95% CI) | LR− (95% CI) | OR (95% CI) | |
|---|---|---|---|---|---|---|
| Δp LDH>0% | 70 (49–84) | 72 (61–81) | 72 (62–80) | 2.5 (1.6–4) | 0.42 (0.22–0.79) | 6 (2.2–16.6) |
| Δp neutrophils>−10%b | 73 (52–87) | 51 (40–62) | 56 (46–65) | 1.5 (1–2.1) | 0.54 (0.26–1) | 2.7 (1–7.8) |
| Δa proteins<0.1g/dL | 83 (63–93) | 37 (27–48) | 47 (38–57) | 1.3 (1–1.7) | 0.47 (0.19–1.21) | 2.8 (0.9–9) |
| Δp LDH>0% and Δp neutrophils>−10%b and Δa proteins<0.1g/dL | 55 (35–73) | 89 (81–95) | 82 (73–88) | 5.2 (2.4–11.1) | 0.51 (0.32–0.81) | |
| Δp LDH>0% or Δp neutrophils>−10%b or Δa proteins<0.1g/dL | 87 (68–95) | 33 (24–45) | 46 (36–56) | 1.3 (1–1.6) | 0.39 (0.13–1.18) |
95% CI: 95% confidence interval; Δa: absolute difference; Δp: percentage difference; LDH: lactate dehydrogenase; LR: likelihood ratio; OR: odds ratio.
Our study shows that a sample of lymphocytic exudate that is negative in the first cytology study is more likely to be malignant if the following three features are observed in a second biochemical analysis: Δp LDH>0%, Δp neutrophils>−10% and Δa proteins<0.1g/dL.
Several studies have attempted to identify predictors of malignant PE. Harris et al.9 studied a series of 198 thoracoscopies (98 patients with malignant PE and 100 with benign PE). They found that patients with malignant PE more often had a history of cancer, were over 50 years of age, and presented bloody PE with higher concentrations of LDH (647U/L vs 192U/L vs 308U/L in malignant PE, idiopathic PE, and other benign PE, respectively, P=.02). Ferrer et al.6 subsequently published a series of 93 thoracoscopies performed in patients with PE of uncertain etiology after at least one cytological and biochemical study of PF, an X-ray and a chest CT scan. Thoracoscopy revealed cancer in 50 cases. Predictors of malignant PE as opposed to benign etiologies (mainly idiopathic PE or benign asbestos PE) were: chest CT suggestive of cancer, bloody PF, history of symptoms longer than 30 days, and no fever. If all four conditions were met, the AUC for identifying malignant PE was 0.95 (95% CI: 0.91–0.99). However, six patients who had been classified as benign by thoracoscopy (as well as according to the analysis of predictors) developed cancer during follow-up. Alemán et al.10 did not identify any biochemical parameter in PF that would help differentiate between malignant and idiopathic PE, but they evaluated only one thoracentesis.
Chung et al.11 performed thoracenteses on three consecutive days in 26 patients with malignant PE, in order to evaluate the effect of this procedure on PF characteristics. Like us, they found a decrease in protein levels and an increase in neutrophils, suggesting that the thoracentesis in itself induced an inflammatory effect. This study did not include other groups with PE of different etiology. Our hypothesis is that benign PEs (mainly tuberculosis, idiopathic, or pericarditis in our study) have a pathological origin that gradually resolves, and this may neutralize the inflammatory effect of the thoracentesis procedure and, thus, cause the LDH and neutrophils to fall.
The same group of investigators repeated the experiment in 21 patients with PE caused by heart failure and found a significant increase in LDH, red blood cells, white blood cells and neutrophils between the second and third thoracentesis.12 It had already been reported that in heart failure, diuretic treatment extracted more water than solutes from the PF, and probably also cells, leading to an increase in LDH in the second thoracentesis.13
Idiopathic PEs are often investigated with a large number of diagnostic techniques, despite the fact that most (more than 91% and 96% in two series of 75 and 53 patients) are due to benign disease.14,15 This finding would support a conservative attitude and underlines the importance of identifying predictors of idiopathic PE that might obviate the need for unnecessary invasive procedures.
Our study has limitations. It is retrospective with a small sample size, since we prioritized patients that presented the greatest diagnostic challenge16: individuals with lymphocytic exudates that tested negative for malignancy in the first cytology test, who then underwent a second thoracentesis, as recommended by guidelines for the management of PE.1,17 Furthermore, different laboratory techniques were used during the course of the study for the measurement of the biochemical parameters of PF which are, in turn, liable to inter-assay (reproducibility) and intra-assay (repeatability) variations. This, however, did not affect the final results, because even if differences were observed between these parameters, the same laboratory techniques were always used in both thoracenteses. Finally, the relative proportion of idiopathic PEs in the derivation population and the validation population differed (20.5% and 6%, respectively), and this may explain why the presence of all three relevant biochemical variables did not achieve a clinically significant negative LR.
One example of the practical relevance of the results may be the following: if the pre-test probability that a predominantly lymphocytic PE is malignant is approximately 24%,2 a second thoracentesis that, compared to the first, shows a percentage increase in pleural LDH levels (or a reduction of less than 10%), along with an absolute reduction in proteins (or a reduction of less than 0.1g/dL), raises this probability to 64% (LR=5.6). In contrast, if the second thoracentesis does not meet any of the foregoing characteristics, the probability of malignancy would fall to 1.2% (LR=0.04).
In conclusion, the finding of an increase in Δp LDH and Δp neutrophils, along with a fall in Δa proteins in PF in a second thoracentesis in a patient whose first thoracentesis showed a lymphocytic exudate of uncertain etiology, is a sound basis for performing the invasive procedures required to reach a definitive etiological diagnosis. However, a fall in Δp LDH or Δp neutrophils, or an increase in Δa proteins would probably justify a more conservative search for a diagnosis.
Conflict of InterestThe authors state that they have no conflict of interests.
Please cite this article as: Bielsa S, García-Zamalloa A, Monteagudo P, González-Sans D, Ascanio D, Esquerda A, et al. Cambios en los parámetros bioquímicos del líquido pleural entre 2 toracocentesis consecutivas para diferenciar derrames malignos de benignos. Arch Bronconeumol. 2018;54:320–326.







