
Various studies have analyzed the presence of comorbidities and risk factors in patients with COVID-19. It is interesting to note that the frequency of chronic respiratory diseases varies widely in different countries. The number of patients with asthma and chronic obstructive pulmonary disease (COPD) in case series from hospitals in China and Italy were much lower than expected for the prevalence of these diseases.1–4 In New York and the UK, however, the frequency is much higher.5,6
In a series of 140 SARS-CoV-2 patients hospitalized in Wuhan, no cases of asthma were described, and only 1.4% had COPD.1 In another multicenter series from the same country that included 476 patients with COVID-19, 4.6% had COPD, but asthma was not mentioned among the comorbidities.2
In a systematic review of the prevalence of comorbidities in patients with COVID-19, also in China, Yang et al.3 observed respiratory diseases in only 1.5% of patients. Similar results have been reported in Italy; in a series of 1,591 patients with COVID-19 seen in critical care units, 4% had COPD, but the asthma figure was so low that it is not mentioned individually.4 This, however, contrasts starkly with data from the US and the UK.
In a series of 5,700 patients hospitalized in New York, 9% had asthma and 5.4% had COPD.5 The figures in the UK are even higher: 19% of patients had non-asthmatic chronic pulmonary disease, and 14% had asthma6 (which has a prevalence of 6.5% in the UK7), suggesting that these comorbidities are very significant risk factors.
The conflicting findings in the prevalence of chronic respiratory diseases in patients with COVID-19 in different countries, and the possibility that these diseases or their treatment may modify the risk of SARS-CoV-2 infection, have prompted us to analyze this situation in our setting. We performed a retrospective observational study of cases admitted to our hospital with a diagnosis of COVID-19 to establish the frequency of asthma and COPD. The study was approved by the local ethics committee.
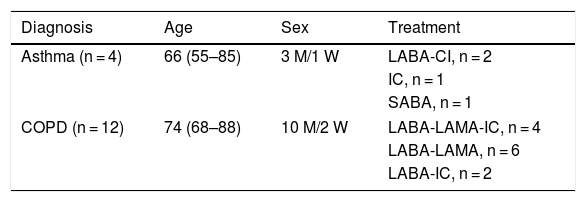
The electronic medical records of 168 consecutive adult patients (aged over 14 years) admitted for COVID-19 were reviewed, and a diagnosis of asthma or COPD was established when it had been recorded by an attending physician in the medical record, regardless of the diagnostic techniques used. We also recorded the number of active prescriptions for inhaled drugs. The age of the patients (median, interquartile range) was 66 years (54–77) and 66 were women (39%). Four patients (3 men) were diagnosed with asthma (2.4% of those admitted). Twelve patients (10 men) had a diagnosis of COPD (7.1% of those admitted). Table 1 shows the demographic characteristics of the sample.
Patients diagnosed with asthma and COPD.
| Diagnosis | Age | Sex | Treatment |
|---|---|---|---|
| Asthma (n = 4) | 66 (55–85) | 3 M/1 W | LABA-CI, n = 2 |
| IC, n = 1 | |||
| SABA, n = 1 | |||
| COPD (n = 12) | 74 (68–88) | 10 M/2 W | LABA-LAMA-IC, n = 4 |
| LABA-LAMA, n = 6 | |||
| LABA-IC, n = 2 | |||
COPD: chronic obstructive pulmonary disease; IC: inhaled corticosteroids; LABA: long-acting beta-adrenergic bronchodilator; LAMA: long-acting muscarinic antagonist; M: men: SABA: short-acting beta-adrenergic; SAMA: short-acting muscarinic antagonist; W: women.
Age expressed as median and range (minimum, maximum).
The prevalence of asthma and COPD observed in our series is similar to that of the general population in Spain (around 2%–3% for asthma8 and 10% for COPD in individuals aged over 40 years, although this disease is frequently underdiagnosed9). Our prevalence rates are somewhat higher than those described in China and Italy, but much lower than the US and the UK. Based on our experience with other respiratory viruses, we would expect a higher proportion of hospitalized patients with asthma and COPD, and there is evidence that patients with chronic respiratory diseases have a very high risk of requiring hospital admission for viral processes that are spread via the respiratory tract, such as seasonal influenza.10,11 In addition, patients with COPD could be suspected of being more susceptible to SARS-CoV-2 infection because the virus uses the angiotensin-converting enzyme 2 (ACE-2) receptor as its route of entry, and expression of this enzyme is increased in patients with COPD.12 However, in our series, only 4 patients had asthma, almost all of whom were men and none were younger than 55 years of age – figures that do not reflect the prevalence of this disease in the general population. These characteristics, together with those described in other series, could lead us to suspect that some asthma patients in Spain may be less susceptible to SARS-CoV-2 infection and COVID-19. It has been suggested that the low reported prevalence of chronic respiratory disease (especially asthma) in the series from China and Italy could be explained by 3 factors: poor recognition (which seems unlikely); a protective effect due to an immune response; and finally, a possible effect of the treatment given for these diseases.13 We cannot rule out the possibility that patients with respiratory diseases will have taken precautionary measures (in some countries but not in others, in view of the differences described) to avoid exposure to the virus, and therefore have a lower risk of contagion.
The possibility that inhaled treatment influences the risk of SARS-CoV-2 infection is not based solely on prevalence data among those admitted with COVID-19. In in vitro models, inhaled corticosteroids (alone or in combination with bronchodilators) have been shown to suppress coronavirus replication and cytokine production.14 Therefore, it could be interesting to evaluate whether the use of these drugs could have a protective effect against SARS-CoV-2.
In conclusion, patients with asthma or COPD in our setting do not seem to be at higher risk of admission for COVID-19. Our data show that the prevalence of asthma or COPD among patients admitted for COVID-19 is similar to that estimated in the general population, and significantly lower than our experience with other respiratory viral diseases would lead us to expect.
FundingThe authors have not received funding for this study.
Please cite this article as: García-Pachón E, Zamora-Molina L, Soler-Sempere MJ, Baeza-Martínez C, Grau-Delgado J, Padilla-Navas I, et al. Asma y EPOC en pacientes hospitalizados por COVID-19. Arch Bronconeumol. 2020;56:604–606.







