


Airway remodeling (AR) with chronic inflammation, are key features in asthma pathogenesis. AR characterized by structural changes in the bronchial wall is associated with a specific asthma phenotype with poor clinical outcomes, impaired lung function and reduced treatment response. Most studies focus on the role of inflammation, while understanding the mechanisms driving AR is crucial for developing disease-modifying therapeutic strategies.
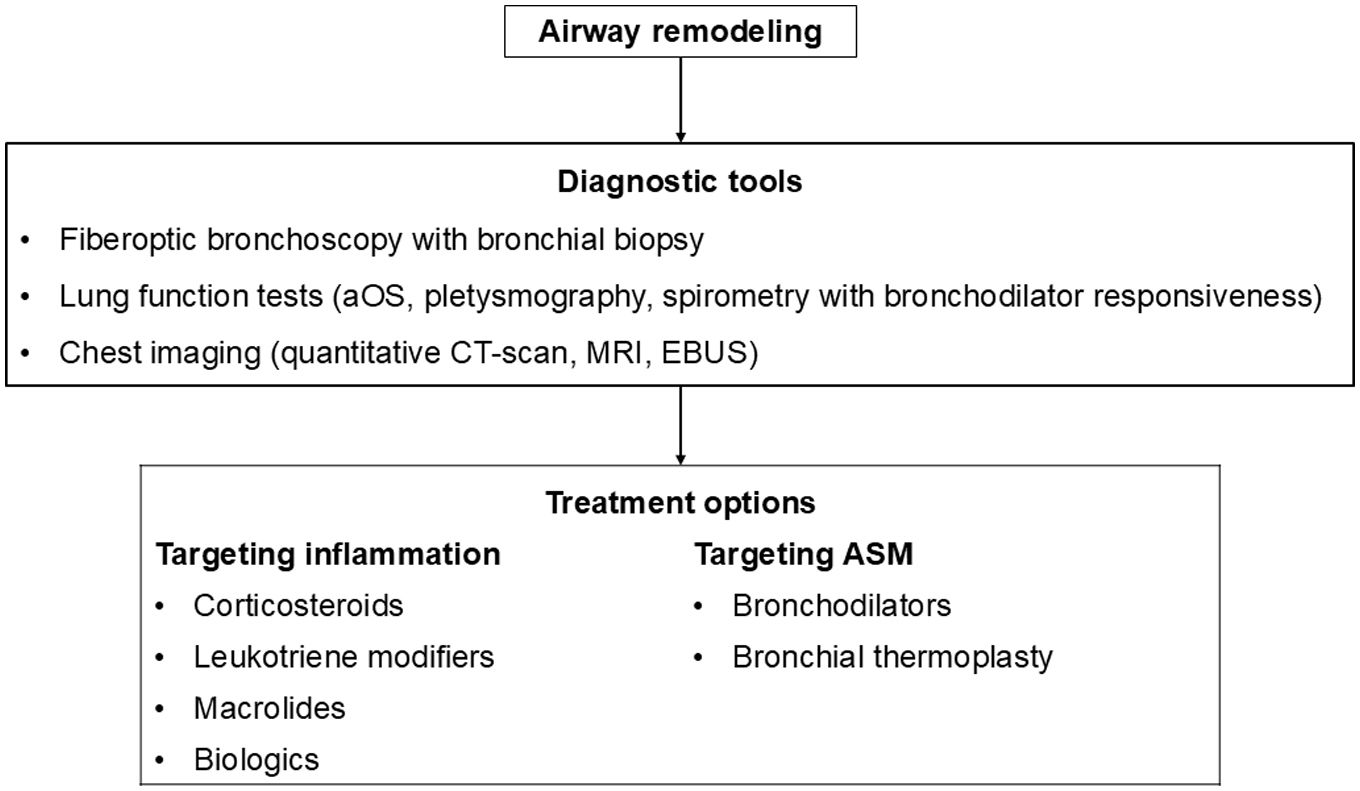
This review paper summarizes current knowledge on the mechanisms underlying AR, diagnostic tools, and therapeutic approaches. Mechanisms explored include the role of the resident cells and the inflammatory cascade in AR. Diagnostic methods such as bronchial biopsy, lung function testing, imaging, and possible biomarkers are described. The effectiveness on AR of different treatments of asthma including corticosteroids, leukotriene modifiers, bronchodilators, macrolides, biologics, and bronchial thermoplasty is discussed, as well as other possible therapeutic options.
AR poses a significant challenge in asthma management, contributing to disease severity and treatment resistance. Current therapeutic approaches target mostly airway inflammation rather than smooth muscle cell dysfunction and showed limited benefits on AR. Future research should focus more on investigating the mechanisms involved in AR to identify novel therapeutic targets and to develop new effective treatments able to prevent irreversible structural changes and improve long-term asthma outcomes.
Asthma is a chronic airway inflammatory disease characterized by typical respiratory symptoms (cough, wheeze, chest tightness, shortness of breath) that vary over time and in intensity associated with variable expiratory airflow limitation. In some patients with long-lasting asthma, airflow obstruction becomes persistent and incompletely reversible due to pathological airway remodeling (AR).1,2
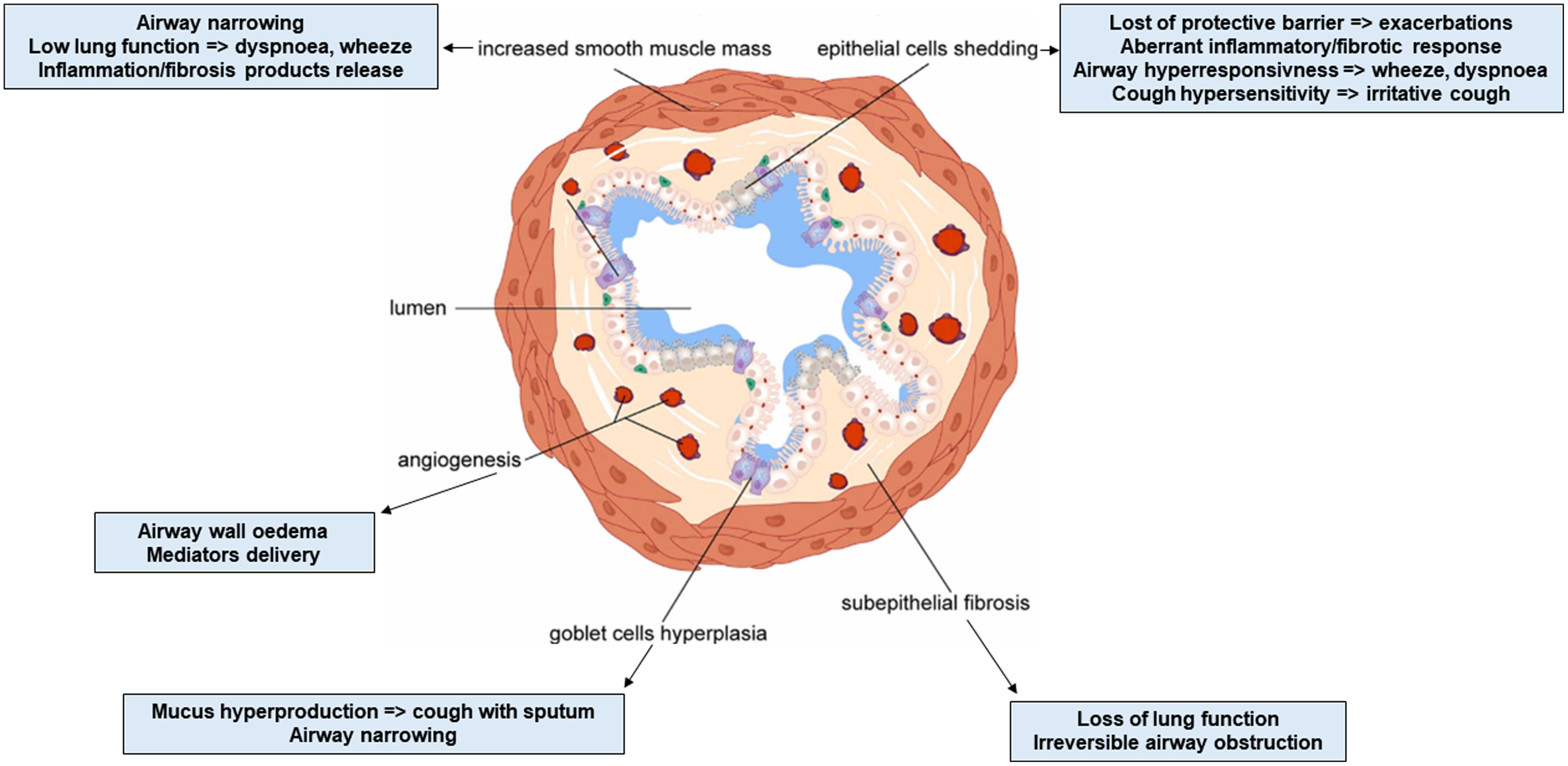
AR is a complex feature of asthma that involves long-term changes of airway architecture such as hyperplasia of the smooth muscles, subepithelial collagen deposition with increased thickness of the reticular basement membrane (RBM), disruption of the epithelial barrier integrity with metaplasia of goblet cells inducing mucus hyperproduction, and angiogenesis.3,4 AR pathogenesis is not fully understood. Until recently, it was thought that it is caused by chronic airway inflammation.5 However, AR is not only a feature of late-onset asthma, because structural changes were found in bronchial biopsies from pre-school children with severe wheezing and a murine model with neonatal inhaled allergen-disease.6–8 These findings suggest that AR may occur early in the disease, and could be a triggering process, rather than a secondary event.9,10 A genetic predisposition is also suggested.4 AR is associated with poor clinical outcomes, impaired lung function, lower response to treatment, and altered quality of life (measured by Asthma Quality of Life Questionnaire – AQLQ) in asthma patients.11 Even though the degree of remodeling correlates with asthma severity, alterations of the bronchial wall are also present in mild disease.12,13 Like inflammation, AR in asthma is heterogeneous, varies between individuals, and may contribute to asthma phenotypes and endotypes.14
As the presence of AR is associated with more severe asthma (SA) and poor response to treatment, targeting this component of the disease with early diagnosis and prevention could improve clinical outcomes and patients’ AQLQ score.13 This review summarizes current knowledge on the mechanisms underlying AR in asthma, the diagnostic tools, the clinical phenotypes and the possible therapeutic approaches in the aspect of personalized medicine.
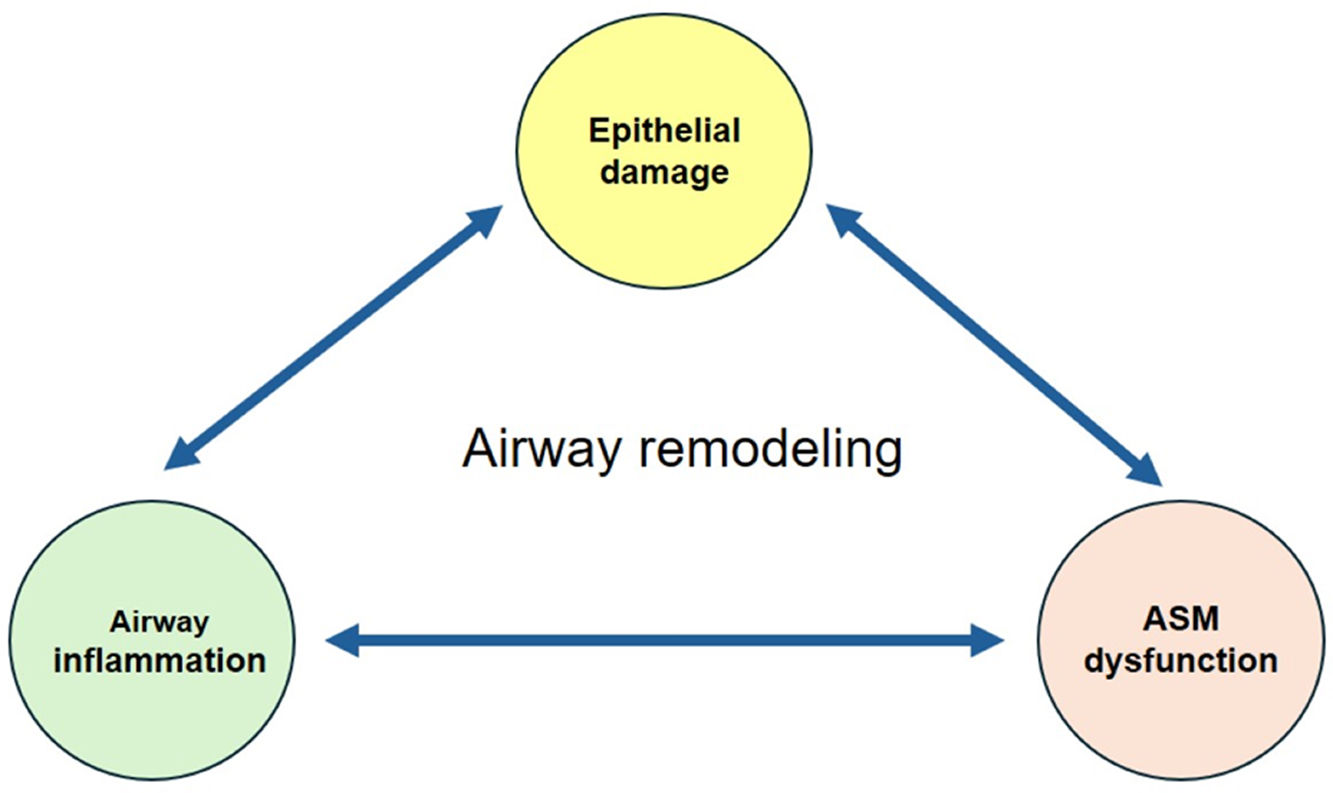
MechanismsAR is the result of complex interaction between the airway resident cells (epithelial cells, smooth muscle cells, fibroblasts, neuronal cells, endothelial cells), the inflammatory cells (dendritic cells – DCs, eosinophils, neutrophils, mast cells – MCs, macrophages, lymphocytes and innate lymphoid cells – ILC), and many humoral components (cytokines, enzymes, and growth factors)2,7,10 (Figs. 1 and 2).


Mechanisms involved in asthma airway remodeling. AHR: airway hyperresponsiveness, ASM: airway smooth muscle, BL: B lymphocyte, DC: dendritic cell, Eo: eosinophil, EMT: epithelial mesenchymal transition, Fbs: fibroblast, FMT: fibroblast–myofibroblast transition, IL: interleukin, ILC2: innate lymphoid cell type 2, Mϕ: macrophage, MC: mast cell, MMP: matrix metallo-proteinase, Mfbs: myofibroblast, Ne: neutrophil, Th2: T helper 2 cell, Th17: T helper 17 cell, TGF-β: transforming growth factor beta.
According to the “inflammatory theory”, the airway epithelial cells (AECs) are the “initiators” of the process.10,15 Following exposure to allergens, microbial proteins, and air pollutants, injured AECs release alarmins (e.g. IL-33, IL-25, TSLP) that activate DCs, ILC2, T helper 2 lymphocytes (Th2), MCs, and macrophages, which contribute to downstream inflammation.5,15 In addition, environmental injuries may induce AECs apoptosis, with paracrine secretion of transforming growth factor-β (TGF-β) which initiates tissue regeneration to restore homeostasis. However, persistent, and prolonged tissue stimulation by growth factors can lead to pathological AR seen in asthma.10
The alarmins could directly induce collagen production by lung fibroblasts. IL-25 promotes lung fibroblasts proliferation while IL-33 induces the expression of fibronectin. The consequent accumulation of extracellular matrix (ECM) proteins leads to subepithelial RBM thickening that occurs early in the pathogenesis of asthma.15
The three alarmins promote eosinophilic inflammation by activating ILC2 and Th2 via DCs, both sources of IL-4, and IL-13, that increase mucus production, collagen synthesis and deposition, airway smooth muscle (ASM) cell contraction and proliferation, and fibroblast-to-myofibroblast transition (FMT).15,16 Eosinophils release various mediators including TGF-β that can directly activate the AECs and mesenchymal cells.15 Alarmins trigger the production of TGF-β by macrophages and stimulate ASM proliferation. Activated macrophages release matrix metalloproteinases (MMPs) that can alter the ECM structure.10,15 During allergic response, MCs secrete mediators (e.g. histamine, prostaglandin D2, tryptase), cytokines (e.g. TSLP, IL-33, IL-13), and vascular growth factors that induce fibroblast, endothelial, and epithelial cell proliferation promoting AR.13 In non-allergic asthma, AECs stimulate the production of Th17 cytokines inducing neutrophilic inflammation and TGF-β production with accumulation of fibrotic matrix components. The immune cells are “amplifiers” of AR.10
The epithelial–mesenchymal transition (EMT), a key feature of AR, is a biological process allowing AECs to assume a mesenchymal cell phenotype. That includes increased migratory capacity, invasiveness, resistance to apoptosis, and production of ECM components, contributing to airway wall fibrosis.10 This process is upregulated by growth factors (e.g. TGF-β), cytokines and mediators (e.g. IL-4, IL-24, MMPs) secreted by resident and inflammatory cells.17–21
Subepithelial fibrosis is mediated by submucosal resident fibroblasts that proliferate and differentiate into myofibroblasts through the process of FMT. Myofibroblasts are mesenchymal cells with contractile and secretory abilities (e.g. collagen, fibronectin, MMPs, growth factors). TGF-β plays a central role in the induction of FMT in asthma, but interleukins (e.g. IL-4, IL-5, IL-13, IL-17, IL-25, IL-33), chemokines (eotaxin, periostin), as well as mechanical forces and ECM proteins could also influence this process.22
ASM mass is increased in both large and small airways in asthma due to cells hyperplasia. The ASM layer thickness correlates positively with the severity of asthma. Additional immigration of myofibroblasts contributes to the rise of ASM layer. These processes are triggered by growth factors (e.g. TGF-β), cytokines (e.g. TSLP), components of the ECM, and chemokines.23 ASM cells from asthma patients exhibit increased metabolism, and proliferation which can lead to changes in mechanical capabilities, increased airway stiffness, and the formation of mucosal folds.14 ASM cells can also contribute to airway inflammation through the release of cytokines and chemokines (e.g. IL-5, IL-13, eotaxin), regulate ECM via the secretion of MMPs, collagen type I, and perlecan, which in turn, may promote the ASM proliferation. MCs infiltration is increased in ASM in asthma patients, and their number correlates with the degree of airway hyperresponsiveness (AHR).13 In this model, fibroblasts and ASM cells are “effectors” of AR in asthma.10
AR as Primary EventASM is the cell responsible for generation of airway tone and contraction. Enhanced contractility of ASM was found in asthma patients due to abnormalities of calcium homeostasis and/or sensitization and altered airway innervation. Increased ASM contractility contributes to AHR.24 AR might be initiated in the absence of inflammation, following bronchoconstriction in response to stimuli.2,7 During bronchoconstriction, the airway epithelium is subjected to excessive mechanical forces causing AECs damage that leads to previous described effects contributing to AR (e.g. release of TGF-β promoting subepithelial fibrosis by fibronectin collagen type III and V deposition, FMT, ASM cells hyperplasia and mucus hypersecretion due to goblet cell metaplasia). Bronchoconstriction stimulates epithelium to release IL-6, IL-8, and monocyte chemoattractant protein-1, which act as mitogens for ASM cells.13 Several data suggests that mitochondrial dysfunction could play a role in ASM remodeling in asthma.8,25
Diagnosis ToolsBronchial BiopsyThe gold standard of AR diagnosis requires bronchial biopsy by fiberoptic bronchoscopy allowing to the direct examination of the tissue (Fig. 4). However, this method is invasive and reflects mostly the proximal airways rather than small airways, so it is not recommended to be performed routinely in clinical practice.2,10 A recent study in asthma adults identified different clusters according to the structural changes on bronchial biopsies. The cluster with high ASM mass (19% of studied patients) was characterized by sputum eosinophilia, elevated total serum IgE levels, increased prevalence of positive skin test for Aspergillus sp, low lung function, important AHR, and moderate therapeutic pressure. The particularities of the cluster with high RBM thickness (31% of patients) were: increased prevalence of atopy, high total serum IgE levels, sputum eosinophilia, moderate decrease in lung function, elevated exhaled fraction of nitric oxide (FeNO) despite maximal daily doses of inhaled corticosteroids (ICS), and great AHR.26 Asthma patients with ASM area>26.6% had worse asthma control, high rate of exacerbations per year and increased weekly use of reliever medication.25


Currently there are no specific biomarkers for the assessment of AR in clinical practice. Blood eosinophilia was identified as a risk factor for airflow obstruction in asthma and predictive for enhanced longitudinal decline in lung function.27 Clinical studies showed increased levels of eosinophils in blood, sputum, and bronchoalveolar lavage fluid in patients with irreversible airway obstruction (IRAO) compared to those with reversible airway obstruction.28,29 FeNO, another biomarker of T2-asthma, is correlated with greater AHR in asthmatic children and adults.27 Elevated serum levels of periostin were found in asthma adults with fixed and more severe airflow obstruction, while its expression in bronchial biopsies is associated with enhanced lung function decline.27–29 Serum periostin seems to be more useful than blood eosinophils or FeNO for assessing AR in asthmatics, even in those well-controlled.30,31 Patients with IRAO have high serum levels of fibrinogen and TGF-β, but their potential as biomarkers of AR should be better investigated.28,29
Lung Function TestsAsthma diagnosis is usually confirmed when evidence of variable expiratory airflow limitation assessed by spirometry or measure of Peak Expiratory Flow (PEF), over time, and in magnitude. Spirometry testing allowed to the measure of the forced expiratory volume per second (FEV1) and the ratio of FEV1 to forced vital capacity (FEV1/FVC). Decrease of these parameters indicates expiratory airflow limitation. Responsiveness (previously called “reversibility”) should be tested if suspicion of asthma. Improvement from baseline in FEV1 or FVC by ≥12% and 200mL, measured within minutes after inhalation of rapid-acting bronchodilator, or weeks after the introduction of ICS was considered longtime as a positive responsiveness test, but recently the cut-off has been changed by >10% of the patient's predicted value. Sometimes, a bronchial provocation test is needed to assess AHR.1
Some asthma patients develop IRAO (FEV1/FVC<0.7 and FEV1<80%) due to the presence of AR.24,25 They have a particular clinical phenotype of “asthma with persistent airflow limitation”1 (Fig. 3). IRAO is present in 55–60% of patients with SA.10
PEF measurement is not useful for the diagnosis of AR. Spirometry assesses the severity of airflow obstruction, but it not directly detects AR. However, certain spirometry findings like the persistent airflow limitation despite treatment, the reduced lung function, and the decreased responsiveness to bronchodilator medications may suggest the presence of AR in severe or long-standing asthma. Spirometry is useful for monitoring disease progression in asthma, including AR development over time, and helps physicians to prevent this feature by adjusting the treatment.1 In addition to spirometry, the plethysmography assesses the airway resistance (Raw) directly related to AR and the presence of indirect signs of airway obstruction such as pulmonary hyperinflation.29,32,33 The bronchial lumen area correlates directly with bronchial obstruction parameters (FEV1, forced mid-expiratory flow FEF25–75) and inversely with residual volume and Raw.33 Airway oscillometry (aOS) is particularly useful in asthma. By measuring Raw, reactance, and impedance across a range of frequencies, aOS provides a more comprehensive evaluation of airway function compared to traditional spirometry. Increased Raw and respiratory impedance correlate with the degree of AR in asthma and could detect early changes in airway function even before airflow limitation.34 Oscillometry bronchodilator response also seems more sensitive than those assessed by spirometry and should be performed before labeling people with the term IRAO.35 Persistent AHR has been identified as a risk factor for longitudinal decline of FEV1 in asthmatics even in those well-controlled by ICS.36 Early identification of AHR by bronchial provocation tests allows for timely therapeutic intervention and prevention of AR.1
Several factors were identified as associated with IRAO such as male gender, long disease duration, cigarette smoking, uncontrolled asthma, sputum eosinophils and neutrophils, and high therapeutic pressure including oral corticosteroids (OCS). An Asthma Control Questionnaire score of 2.36 could identify IRAO with a high sensitivity (72%) and specificity (77%).28
ImagingRoutinely performed chest X-ray examination is not helpful to evaluate AR in asthma patients. Its clinical value is restricted to identify asthma complications or concomitant disorders such as pneumonia or pneumothorax.
The airways have been reliably examined with computed tomography (CT) scans from more than 20 years.37,38 Since its introduction, multidetector computed tomography (MDCT) has proved to be particularly useful in the evaluation of AR in asthmatic patients.39–41 By applying minimal radiation levels, the new-generation MDCT provides better resolution than helical CT with acquisition of multiple cross-sectional slices as thin as 0.60–0.75mm without interslice gaps, in shorter time, during inspiratory and expiratory phases, with the possibility to extract quantitative data.42–45 Quantitative CT (qCT) can evaluate bronchial thickness (lumen diameter – LD and area – LA, bronchial wall thickness – WT and area – WA), the presence of mucous plugs in the airways, lung hyperinflation and air trapping (e.g. identification of low-attenuation areas, measure of lung density).39,46–49 The features of AR observed in qCT images show strong correlations with pathological and functional examinations.29,50,51 Analysis of qCT allowed to identify distinct asthma phenotypes with different clinical outcomes. The more advanced AR on qCT is associated with low lung function, high exacerbation rate, and worse response to standard therapy.29,47,52 Mucus plugging on CT-scan is linked to T2-inflammation, more severe asthma, frequent exacerbations and poor lung function.53,54 Positive correlations were found between WA%≥50% on CT-scan and increased peripheral resistance and reactance measured by aOS.55 Recent longitudinal studies demonstrated that qCT can help in selecting asthmatics prone to irreversible loss of lung function with time and assist in the evaluation of response to biologics, becoming a useful diagnostic tool for personalized medicine in asthma management.46,56,57
Compared to CT-scan, magnetic resonance imaging (MRI) provides superior soft-tissue contrast, without patient radiation exposure.58,59 Fast imaging protocols are based on breath hold acquisitions or triggering/gating to compensate for motion artifacts.59 However, MRI has lower spatial resolution than qCT, so non-contrast-enhanced MRI is not very useful for the evaluation of subtle changes in airway structure seen in asthma patients.58 The application of hyperpolarized gases with MRI allows to direct assessment of ventilation heterogeneity and quantitative measurement of terminal airway, that correlate with AR. Serial imaging can evaluate disease progression and response to therapy over time.58–60
The endobronchial ultrasound technique (EBUS) is also useful for the assessment of AR in asthma patients.61 EBUS allows the detailed analysis of the bronchial wall structures distinguishing different layers. The inner layers contain the epithelium, submucosa, and ASM while the outer layers correspond to cartilage.61,62 In distal no cartilaginous airways EBUS can visualize the three layers of the bronchial wall.62 The EBUS may be useful for asthma patients to evaluate wall changes after bronchial thermoplasty (BT).63 However, EBUS is an invasive method, requires an expert bronchoscopy skill, and allows for local evaluation of the airways.
The role of other imaging methods such as optical coherence tomography or positron emission tomography in the evaluation of AR should be determined.60,64
TreatmentCorticosteroidsCorticosteroids are the cornerstone of treatment in asthma.1 Several clinical data showed that inhaled corticosteroids (ICS) decreased RBM thickness and collagen type III deposition in bronchial biopsies in asthma patients if administered for more than 6-weeks.65–68 A greater effect was observed after 2-years of treatment with a high-dose of budesonide, suggesting a possible dose-dependent, long-term effect.68 This benefit was not confirmed by all studies with ICS, neither after 2-weeks treatment with OCS.69–72
The data about the effect of corticosteroids on the airway epithelial damage are also divergent. Several experimental studies suggested that corticosteroids may contribute to AR by inducing AECs apoptosis, while others demonstrated that this treatment restored the integrity of epithelial cell monolayers through the redistribution of tight junction proteins.73–75 Bronchial biopsies from asthmatics treated 10-years with ICS showed a significant decrease in the number of inflammatory cells, with small focal areas with non-ciliated cells and persistence of squamous cell metaplasia in some patients, suggesting partial recovery of epithelial damage.76
In an animal model, a single dose administration of beclomethasone caused acceleration of the mucus release from goblet cells probably due to overstimulation.77 Other clinical and experimental studies from asthma patients treated longer time with ICS demonstrated an increase in the number of ciliated cells and a reduction of goblet cell hyperplasia suggesting a possible time-dependent effect.78,79
On asthma patients, a 6-months treatment with inhaled beclomethasone dipropionate decreased both vessel number and percent vascularity within the lamina propria, modifications associated with changes in collagen III thickness.80 Another study showed a significant reduction in the vascular component of AR only in asthma patients receiving high-dose inhaled fluticasone propionate after 6-weeks of treatment.81
Despite undeniable evidence of ICS effectiveness on reducing AHR, the therapeutic index is not the same for all products and some asthma patients under treatment continue to have airflow obstruction.65,69,82–84 In addition, the long-term use of high-dose ICS is associated with potential systemic side effects.85
Beta-agonistsBeta-agonists are vital for alleviating asthma symptoms by relaxing ASM.1 Experimental data suggests that long acting β2-agonists (LABA) have no impact on ASM cells hyperplasia in asthma patients, but the association ICS-LABA decreased goblet cell metaplasia.86,87 A clinical study showed that salmeterol addition in asthmatics already receiving ICS, reduced vessels density in lamina propria after 3-months of treatment.88
AnticholinergicsStudies on animal models suggested that tiotropium administration could reduce AHR, mucus production, thickness of ASM, subepithelial fibrosis, and goblet cell metaplasia.89–91 Several clinical data showed that addition of tiotropium in asthma patients treated with ICS-LABA significantly decreased airway WA and WT on CT-scan (p<0.05 for both), and improved airflow obstruction, while glycopyrronium offers a better protection against methacholine-induced bronchoconstriction than placebo (p<0.002).92–94
Leukotriene ModifiersIn animal models, leukotrienes receptor antagonists (LTRA) showed a positive impact on AHR, goblet cell hyperplasia, EMT, subepithelial fibrosis, ASM hyperplasia by inhibiting TGF-β signaling.95–101 Zileuton, a leukotriene synthesis inhibitor, reduced ASM mass and ECM deposition in an animal model.102 LTRA improve AHR in asthma patients.103,104 Several clinical data showed that 8-weeks treatment with montelukast prevents AR by decreasing collagen deposition in airways in asthmatic children, and myofibroblast count in adults with mild atopic asthma.98,105
MacrolidesMacrolides are antibiotics recognized for their anti-inflammatory properties, that can reduce exacerbation rate in SA.106 Experimental data suggested that azithromycin administration decreases AECs apoptosis, attenuates goblet cell hyperplasia, suppresses EMT, reduces AHR, proliferation and viability of ASM cells.107–114 Both roxithromycin and azithromycin inhibit vascular endothelial growth factor induced ASM cell proliferation in vitro.115,116 A clinical trial showed that 8-months treatment with azithromycin (250mg three days a week) increased LA in patients with SA on CT-scan without significant change of the WT versus placebo.117
BiologicsBiologics, humanized antibodies used as add-on treatment in patients with SA, showed also benefits on AR.
In vitro administration of the anti-IgE antibody, omalizumab, prevented ASM cell proliferation, collagen and fibronectin deposition in allergic asthma.118,119 Clinical data showed that 16-weeks treatment with omalizumab decreased airway WT on CT-scan in patients with SA.120,121 Effectively, a significant reduction in RBM thickness and fibronectin accumulation was found on bronchial biopsies from patients with severe allergic asthma after 12-months treatment with omalizumab.122,123 The decrease of fibronectin deposition in bronchial mucosa was associated with an improvement in asthma control and AQLQ.123 Experimental and clinical studies demonstrated that omalizumab administration inhibited AHR in allergic asthma.124–126
Biologics targeting IL-5 (mepolizumab) and its receptor α (benralizumab) showed positive impact on AR. One-year treatment with mepolizumab significantly decreased airway WA on CT-scan in patients with refractory eosinophilic asthma.127 Mepolizumab reduced expression of ECM proteins (e.g. tenascin, lumican, procollagen III) and of TGF-β1 by eosinophils in bronchial biopsies from patients with mild atopic asthma, after 3-months of treatment.128 Preliminary results from the MESILICO study showed that one-year treatment with mepolizumab significantly decreased RBM thickness, ASM area, and extent of epithelial damage in patients with late-onset, severe eosinophilic asthma and fixed airflow obstruction.129 Benralizumab reduced the number of tissue myofibroblasts and ASM mass in bronchial biopsies from patients with severe eosinophilic asthma after 3-months of treatment.130 Decrease in mucus plugs and ventilation defects were observed on functional imaging already at day 28 after benralizumab injection in patients with severe eosinophilic asthma, and the early response persisted 2.5-years later, alongside significantly improved asthma control.131–133 Both mepolizumab and benralizumab suppressed the AHR induced by histamine in an experimental study, but this benefit was confirmed only for benralizumab in clinical setting.127,134–136
Experimental data showed that IL-4 receptor α blockade by dupilumab decreased AHR, mucus production, and vascular permeability in the airways.137,138 A prospective clinical study proved that 48-weeks treatment with dupilumab reduced mucus score and airway WT on CT-scan in patients with uncontrolled moderate-to-severe asthma. The decrease in mucus score was associated with improvement of asthma control, AQLQ, and airway obstruction.139
Tezepelumab, an anti-TSLP antibody, showed benefits on AR in a murine model of asthma by reducing collagen deposition, goblet cell hyperplasia, TGF-β levels in the airways, and AHR to methacholine.140 However, a recent randomized clinical trial failed to prove a significant effect of tezepelumab after 28-weeks of treatment on AR assessed by bronchial biopsies, CT-scan and IOS in patients with moderate-to-severe asthma compared to placebo.141 Other clinical data demonstrated a decrease of AHR to mannitol after at least 12-weeks of treatment by tezepelumab versus placebo, and a reduction of occlusive mucus plugs on CT-scan after 28-weeks of treatment.141–143 The last effect was correlated with the improvement in FEV1.143
Other MedicationsAdding six standardized quality house dust mite sublingual immunotherapy to standard pharmacotherapy in patients with allergic asthma and rhinitis for 48-weeks significantly decreased airway WA and WT with increase in LA on CT-scan.144 Fevipiprant, a prostaglandin D2 type 2 receptor antagonist, administered 12-weeks reduced ASM mass on bronchial biopsies in asthma patients by decreasing airway eosinophilia with concomitant diminished recruitment of myofibroblasts and fibrocytes to the ASM bundle.145 Increasing number of studies are focusing on potential therapies that could reduce ASM hypercontractility and AHR by improving abnormalities in calcium homeostasis and in airway innervation.24 A clinical trial showed that gallopamil, a calcium channel blocker, administered for one year, reduces ASM area on bronchial biopsies and normalized ASM thickness on CT-scan.146
Bronchial ThermoplastyBT, an endoscopic treatment using radiofrequency energy, is the only therapy that lastingly decreased AR in 60% of adults with SA.1,147 Besides the reduction in ASM mass, RBM thickening, submucosal nerves, and epithelium neuroendocrine cells, BT induces an ECM rearrangement with increase in tissue area occupied by collagen but a less dense fiber organization.147–151 BT decreased AR by modifying the secretion of epithelium-derived heat shock proteins that improve AECs regeneration with negative impact on fibroblasts and ASM cells proliferation without affecting vasculature.147–149,152,153 Histological parameters were associated with improvement of asthma control, AQLQ, lung function, and reduction of the exacerbation rate.151,154–156 If the response to BT seems to be independent of the bronchodilator responsiveness, the patients with FEV1<80% have a greater reduction in ASM mass after treatment compared to those with higher FEV1.156,157 The reduction in ASM mass by BT becomes visible after 3-months of treatment and could persist>10 years after the procedure.5,151,158
ConclusionAR and chronic inflammation are critical components in asthma pathogenesis. Recognizing that AR may occur early in the disease and not simply as consequence of the inflammation is crucial to developing novel therapeutic strategies in asthma. AR is associated with a specific clinical phenotype of asthma. Understanding the complex mechanisms driving AR is mandatory to identify different pathological endotypes and for developing new therapies in asthma.
Advances in imaging techniques offer the possibility for an objective assessment of AR in the whole respiratory tract in asthmatics by broadly accessible, noninvasive, and highly reproducible tools. Imaging and lung function testing help clinicians to early detect and accurately evaluate the presence of AR in asthma patients.
Most of current therapies of asthma showed limited effects on AR because they are targeting inflammation and not ASM dysfunction. Even BT which acts directly on ASM mass showed benefits only in a selected population. Potential targets causing ASM cell dysfunction were identified, and medications are under study, but more efforts should be deployed on this research way to find effective treatments of AR in asthma.
Funding SourceNone.
Conflict of InterestA.T. received honoraria as speaker for educational events from AstraZeneca, BMS, GSK, and Sanofi; as member of Advisory Board from AstraZeneca and Sanofi; support for attending meetings from AstraZeneca and Sanofi.
P.S. received honoraria as speaker from AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Elpen, Guidotti, Menarini, Specialty Therapeutics; support for attending meetings from AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Elpen, Guidotti, Menarini, Specialty Therapeutics.
S.N. and G.G. have no conflict of interest to declare.
D.N. received honoraria as speaker from AstraZeneca, Berlin Chemie, Takeda, Chiesi and support fro attending meetings from AstraZeneca and Stallergen.
P.N. received honoraria as speaker from Berlin Chemie, Chiesi.
H.C.N. received consulting fees from AstraZeneca, Sanofi; honoraria as speaker from AstraZeneca, Sanofi.
K.K. received royalties from UpToDate, honoraria as speaker from ALK Abello, Aurovitas Pharma, AstraZeneca, Berlin Chemie, Boehringer Ingelheim, Chiesi, EMMA MDT, Stallergenes.
Artificial Intelligence InvolvementNone.







