

A 37-year-old man presented with dyspnea, dry cough and right-sided chest pain for 3 months. Physical examination revealed diminished breath sounds on the right hemithorax with mediastinal shift to left. Chest radiograph showed a right middle and lower zone opacity, and contrast-enhanced computed tomography showed a large heterogenous mass with multiple foci of calcification and necrosis (Fig. 1A and B). An ultrasound-guided biopsy showed features of a cartilage-forming tumor with chondrocytes arranged in lacunae with atypia, features consistent with pulmonary chondrosarcoma (Fig. 1C and D). He progressively worsened and passed away during the hospital stay before any surgery or palliative treatment could be initiated. Pulmonary chondrosarcomas are rare lung tumors that represent less than 1% of primary lung tumors. They present as enlarged, lobulated, or cystic calcified masses. The average age is between 50 and 70 years. It is of two types – tracheobronchial and lung. Immunohistochemistry is positive for S-100, particularly in the chondromatous component.1 Symptoms depend on the size and location of the lesion. Treatment is primarily surgical, with complete resection rates of over 80%. Adjuvant chemotherapy and radiotherapy are recommended for high-grade lesions or incomplete resection. In cases of unresectable tumours, surgery is the primary treatment.2
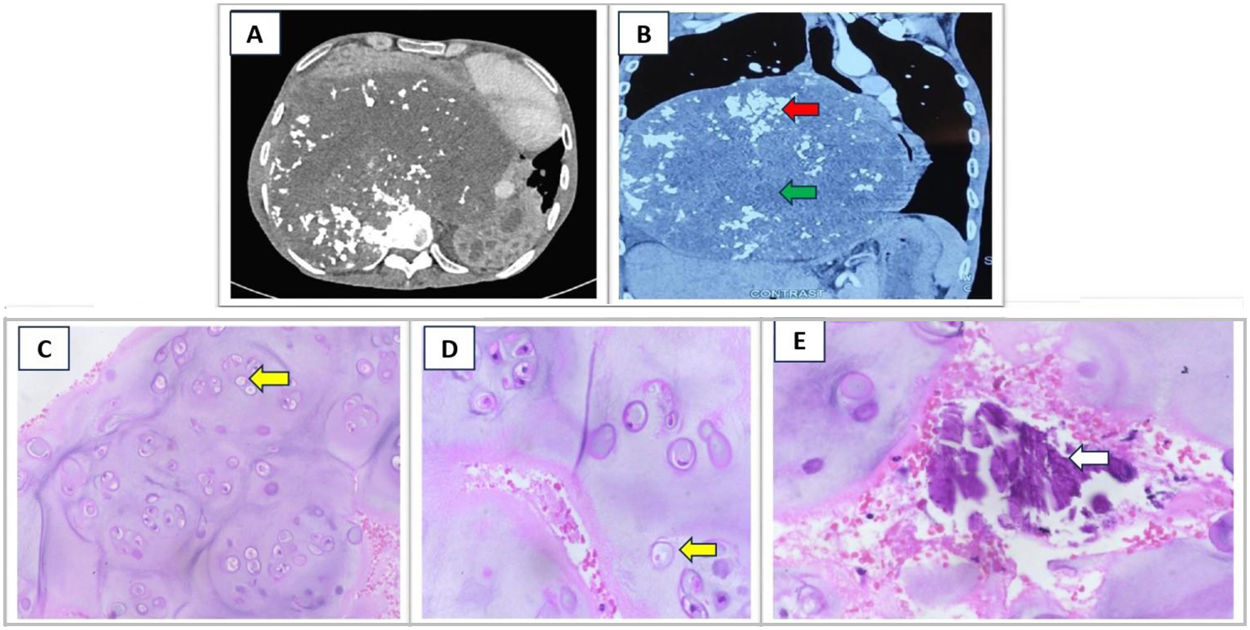
 showing a large heterogenous lung mass in the right hemithorax with focal areas of calcification (red arrow) and necrosis (green arrow), shifting mediastinum to the left. USG guided biopsy of the lung mass was done and the HE-stained images showed the chondrocytes arranged in small clusters, and singly in a lacuna (yellow arrows). There is moderate increase in cellularity with multinucleation, and mild atypia (C – 20×; D – 40×). Image E (40×) shows areas of calcification within the tumour (white arrow).")
CT thorax (A and B – coronal section) showing a large heterogenous lung mass in the right hemithorax with focal areas of calcification (red arrow) and necrosis (green arrow), shifting mediastinum to the left. USG guided biopsy of the lung mass was done and the HE-stained images showed the chondrocytes arranged in small clusters, and singly in a lacuna (yellow arrows). There is moderate increase in cellularity with multinucleation, and mild atypia (C – 20×; D – 40×). Image E (40×) shows areas of calcification within the tumour (white arrow).
There was no involvement of AI in preparation of this manuscript.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of InterestThe authors declare not to have any conflicts of interest that may be considered to influence directly or indirectly the content of the manuscript.







