



(i) To develop sex-specific reference equations to predict distance walked (6MWD) in the 6-minute walk test (6MWT), in healthy subjects aged 45–85 years, from different geographic areas of Spain; and (ii) to compare developed equations with previously published in a large sample of COPD patients.
MethodsFirst, a cross-sectional multicentre sample of randomly selected healthy subjects from 17 Spanish hospitals and universities performed two 6MWT. Linear regression and fractional polynomial modelling were used to develop the equations. Second, the developed equations were applied to 715 COPD patients from Spanish primary care centres and hospitals, and the % predicted 6MWD obtained was compared with previously published equations using Dunnett's multiple comparisons test.
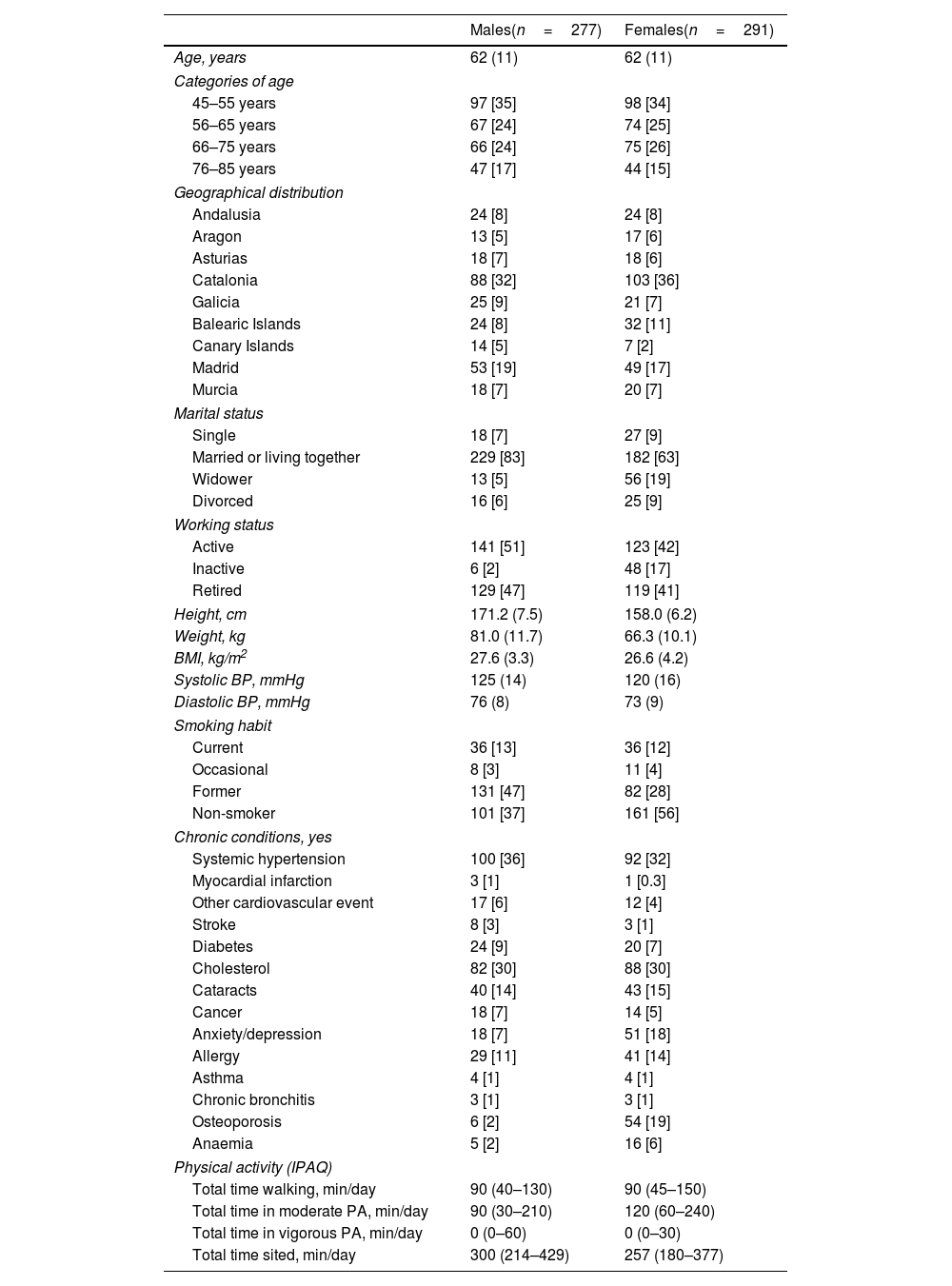
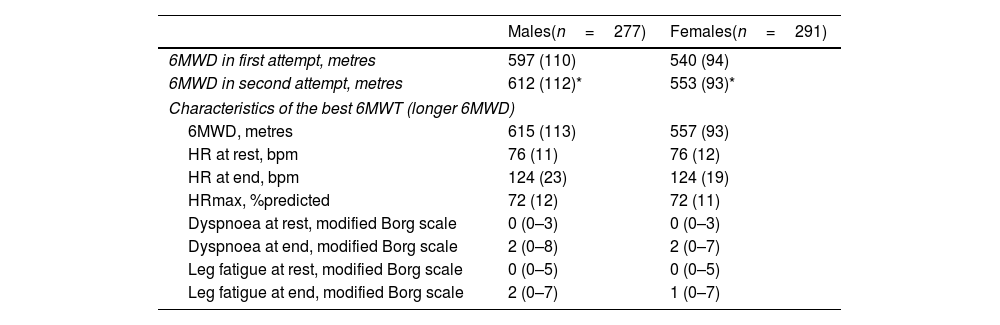
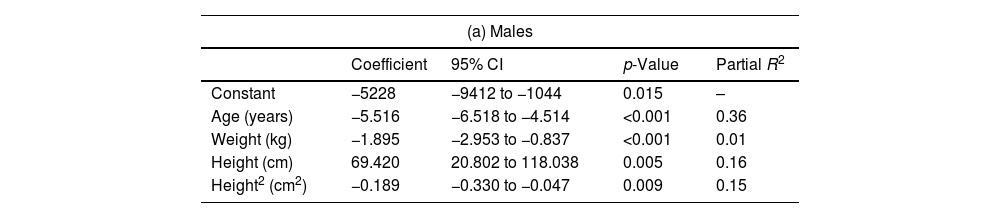
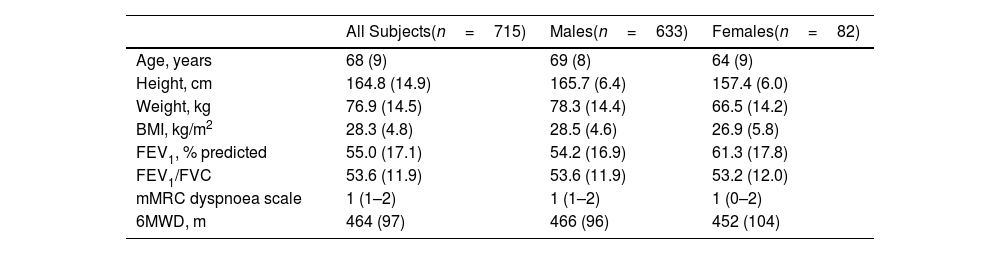
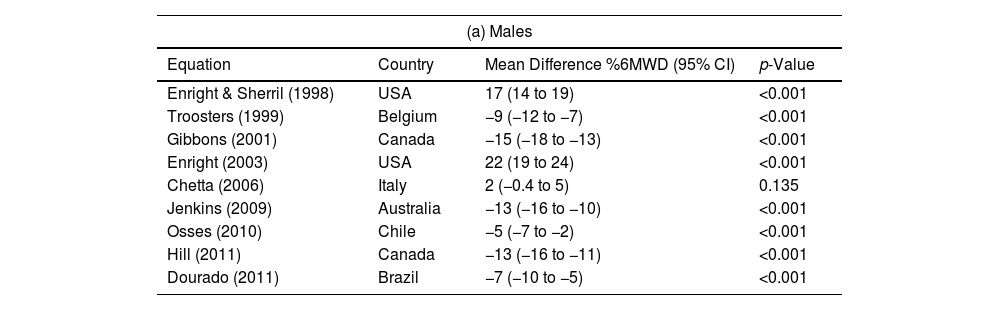
Results568 healthy subjects were included (51% females, mean (SD) age 62 (11) years), walked a 6MWD of 615 (113) and 557 (93)m in males and females, respectively. The developed equations included age, weight and height, and explained 43% and 51% of the 6MWD variance for males and females, respectively. In the COPD sample (n=715, 14% females, 68 (9) years, FEV1 61 (18) % predicted, 6MWD 464 (97)m), only 1 out of 9 previously published equations for males, and 6 out of 9 for females predicted 6MWD values similar to those of the newly developed Spanish reference equations.
ConclusionsThe newly developed reference equations provide a more valid prediction of 6MWD in Spanish adults with COPD compared to previously published equations. We suggest their use in future research and clinical practice for the Spanish adult population.








