





While it is known that asthma symptoms have a very variable pattern, the general belief is that the respiratory symptoms in COPD patients usually present little or no variability. Nevertheless, COPD patients report having “bad days”. The objective of this present study was to evaluate the variability of the respiratory symptoms and their impact on the daily activities of a cohort of Spanish COPD patients.
MethodWe present the results of the Spanish patients who participated in a cross-sectional epidemiological study carried out in 17 European countries. Pulmonologists and Family Care physicians recruited patients with stable severe COPD (FEV1<50%). The perception of the patients on the variation in their symptoms was recorded by telephone interviews.
ResultsA total of 472 patients provided data that were valid for analysis. Mean age was 68.6; 93% were men; mean FEV1(%) was 41%. 84.1% of the patients experimented at least one respiratory symptom in the previous week and 60.9% affirmed that their symptoms varied over the course of the day or week. The moment of the day when the symptoms were perceived to be more intense was during the morning.
ConclusionsAn important proportion of severe COPD patients perceive variability in their respiratory symptoms, with a greater intensity in the morning. The observation can have implications in treating patients with severe COPD as variability can be an initial sign of decompensation of the disease.
Mientras se reconoce que los síntomas en el asma tienen un patrón muy variable, la creencia general es que los síntomas respiratorios en los pacientes con EPOC presentan habitualmente poca o ninguna variabilidad. Sin embargo, los pacientes con EPOC refieren tener «días malos». El objetivo del presente trabajo fue evaluar la variabilidad de los síntomas respiratorios y su impacto en las actividades de la vida diaria en una cohorte de pacientes españoles.
MétodoSe presentan los resultados de los pacientes españoles participantes en un estudio epidemiológico transversal realizado en 17 países europeos. Neumólogos y médicos de familia reclutaron pacientes con EPOC grave estable (FEV1<50%). La percepción de los pacientes sobre la variación de sus síntomas se recogió mediante entrevista telefónica.
ResultadosUn total de 472 pacientes aportaron datos válidos para el análisis. La edad media fue de 68,6 años, el 93% fueron hombres y el FEV1(%) medio fue del 41%. El 84,1% de los pacientes experimentaron al menos un síntoma respiratorio en la semana previa y el 60,9% afirmaron que sus síntomas variaban a lo largo del día o de la semana. El momento del día donde los síntomas se percibían con mayor intensidad fue por la mañana.
ConclusionesUna proporción importante de pacientes con EPOC grave percibe variabilidad de sus síntomas respiratorios, con una mayor intensidad por la mañana. Esta observación puede tener implicaciones para el tratamiento de los pacientes con EPOC grave, ya que la variabilidad puede ser un signo inicial de descompensación de la enfermedad.
One of the differences that is usually used to distinguish asthma from COPD is the variability of the respiratory symptoms. While asthma symptoms have an admittedly very variable pattern, the general belief is that the respiratory symptoms in COPD patients usually present little or no variability.1 In fact, the acute intensification of the symptoms in COPD, known as exacerbations, are defined as a change in the intensity of the symptoms beyond the normal daily variation.2 There are, however, no data to indicate what this supposed daily variation in symptoms is, if it actually exists.
In some studies, patients have reported having “bad days” that do not specifically meet the definition of an exacerbation and which could be interpreted as more symptomatic days.3 The greater intensity of the symptoms may require specific treatment based on short-acting bronchodilators on demand, but it is of greater interest to prevent these fluctuations with the use of long-acting drugs that provide clinical stability. It is also possible that the variability in the symptoms is not a universal characteristic in COPD, but is instead reserved for specific patients with differential characteristics.4 These questions justify carrying out extensive observational studies that would allow us to know the frequency and magnitude of respiratory symptom variability in COPD. A European study has recently been completed that was designed with this aim in mind. It also observed significant differences in the characteristics and the variability of the symptoms between geographical areas.5 These geographical differences in COPD characteristics have previously been mentioned in other studies6,7 and they justify the detailed analysis of the data from different regions. In this context, Spain has participated with a high number of patients in the European study. Although it is an important sample, it cannot be considered representative of the entire Spanish COPD population due to its number and origin from Pulmonology and Primary Care services. It does, however, provide a global perception of the symptoms and their variability in Spanish patients. In the present study, we present the results of the Spanish cohort of the European study with the intention of knowing the variability of the respiratory symptoms in severe COPD and their impact in daily patient life.
MethodsAn observational, epidemiologic, cross-sectional study was done in Spain and in 16 other European countries: Austria, Belgium, Denmark, Finland, France, Germany, Greece, Holland, Ireland, Italy, Norway, Portugal, Sweden, Switzerland, Turkey and the United Kingdom (registry number NCT00722267) with the objective of knowing the variability of the respiratory symptoms and their impact on daily life in patients with severe COPD. The current article only presents the results obtained in the Spanish patients included in the study.
Pulmonologists and primary-care physicians throughout Spain who treated COPD patients on a regular basis were invited to participate in the study. The selection of participants was random and based on a database of physicians from our sponsor. For the inclusion in the study, the patients needed to meet the following criteria: (a) outpatients diagnosed with COPD; (b) age over 45; (c) smokers or ex-smokers of at least 10 pack-years; and (d) severe or very severe COPD defined by an FEV1<50% predicted and an FEV1/FVC<0.7, pre-bronchodilator. The exclusion criteria were: (a) patients who, at the moment of inclusion or within the previous 3 months, had presented exacerbation; (b) history of asthma or rhinitis; (c) lung cancer or other significant respiratory pathology such as bronchiectasis, pulmonary fibrosis, interstitial pathology, tuberculosis or sarcoidosis; (d) participation in a clinical trial; and (e) inability to understand the study procedure or refusal to respond to telephone surveys.
The study was carried out in accordance with the Declaration of Helsinki and was approved by the CEIC of the Hospital Clínic in Barcelona on April 10, 2008 (Register 2008/4181). All the participating patients signed the informed consent.
Data CollectionThe study design and process have been described in detail in a previous publication.5 In short, at the inclusion visit and after signing the informed consent, the researchers collected information about the demographic characteristics of the patients, COPD evolution time, personal history, degree of dyspnea according to the Medical Research Council (MRC) scale,8 exacerbations and previous hospitalizations as well as smoking habit. We also obtained information about the standard medication administered for COPD and for other comorbidities.
Later, the patients were interviewed by telephone with an operator who was independent from the researcher and the study sponsor. The interview entailed answering a survey that was about 20–30min long, during which the patient was asked about his/her COPD symptoms, specifically dyspnea, cough, pressure in the chest, expectoration and wheezing. They were also asked about the variability of the symptoms throughout the day, the week and the seasons of the year, about the quality of sleep, level of tiredness, and the presence of depression or anxiety. Furthermore, they were questioned about the impact of the symptoms on morning activities and at other moments of the day, and also the need for assistance to carry out said activities.
The telephone questionnaire was translated into all the languages used in the study and, prior to its use in the study, its interpretation and comprehension were verified by an independent group of patients in each country. In a previous publication,5 more details can be found regarding the questionnaire, its validation and quality control.
Statistical AnalysisA descriptive study reporting quantitative variables as means and standard deviation. The qualitative variables were described by absolute and relative percentage frequencies. The lost data were not taken into account in the calculation of percentages.
ResultsParticipation and Population CharacteristicsIn Spain, 134 physicians participated (98 [73.1%] pulmonologists and 36 [26.9%] primary care doctors) who included 677 patients. In 128 cases, telephone interviews were not possible (29 refused the interview, 49 had exacerbations, 36 were unable to be contacted, one had died and 13 due to other causes). Out of the 549 patients (81.1%) who were interviewed, 68 had exclusion criteria and 9 provided insufficient data. Therefore, the final study population was made up of 472 valid patients (69.7%).
Mean age was 68.6 (SD: 9.3) and only 33 (7%) were women. Mean pre-bronchodilator FEV1(%) was 41% (SD: 9.9%). 80.5% of the patients presented some type of comorbidity, and the most frequent of these was hypertension (210, 44.5%). On average, the patients had presented 1.97 (SD: 2.3) exacerbations in the previous year, but 32.8% had had none.
All the patients received medication, and the most frequently prescribed drugs were an associated long-acting beta-2 adrenergic (LABA) and an inhaled corticosteroid in 397 cases (84.1%), and long-acting anticholinergics (tiotropium) in 382 (80.9%). The remaining characteristics are shown in Table 1.
Characteristics of the Patients Included in the Study.
| Characteristics | No (%) or Mean (SD) |
| Sex, male | 439 (93) |
| Age, years (SD) | 68.6 (9.3) |
| Active smokers | 73 (15.9) |
| Years since COPD diagnosis | 10 (7.8) |
| Degree of dyspnea | |
| 1 | 29 (6.2) |
| 2 | 208 (44.2) |
| 3 | 139 (29.5) |
| 4 | 80 (17) |
| 5 | 15 (3.2) |
| Comorbidity (with frequency greater than 10%) | |
| Hypertension | 210 (44.5) |
| Ischemic heart disease | 59 (12.5) |
| Diabetes | 87 (18.4) |
| OSAS | 71 (15) |
| Metabolic syndrome | 47 (10) |
| Lung function (pre-bronchodilation values)a | |
| FVC, l | 2.31 (0.66) |
| FVC, % | 67.2 (16.6) |
| FEV1, l | 1.08 (0.31) |
| FEV1, % | 41 (9.6) |
| FEV1/FVC | 47.6 (9.8) |
| Positive bronchodilator test (n=253) | 36 (14.2) |
| Exacerbations in the previous year: mean (SD) | 1.97 (2.3) |
| 0 | 153 (32.8) |
| 1–2 | 178 (38.1) |
| >2 | 136 (29.1) |
| COPD treatment | |
| LABA+IC | 397 (84.1) |
| Long-acting anticholinergics | 382 (80.9) |
| Short-acting bronchodilators | 244 (51.7) |
| Mucolytics | 161 (34.1) |
| Theophyllines | 77 (16.3) |
| Home oxygen therapy | 107 (22.7) |
SD: standard deviation; OSAS: obstructive sleep apnea syndrome; MRC: Medical Research Council scale (positive bronchodilator test defined as an increase in post-bronchodilator FEV1 of ≥200ml and ≥12%; LABA: long-acting beta2 adrenergic; IC: inhaled corticosteroids.
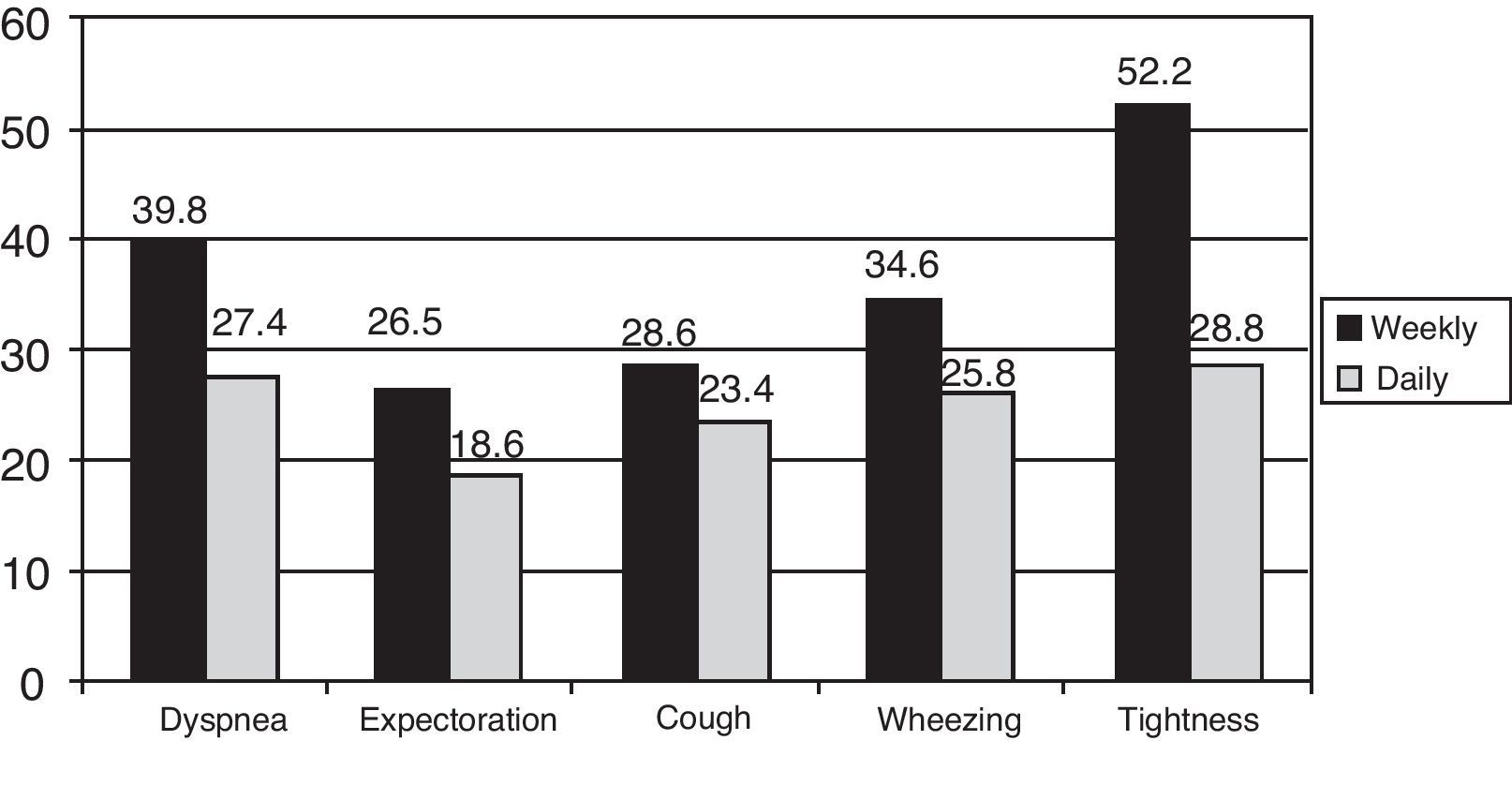
84.1% of the patients declared having at least one symptom in the previous week, and the most frequent was expectoration in 264 cases (55.9%), followed by dyspnea in 235 (49.8%) (Table 2). Out of the patients who responded, 36%–54.9% stated that their symptoms affected them every day of the week (depending on the symptom), while 24.6%–45.9% reported that their symptoms affected them between 1 and 3 days a week (interval between the least frequent and most frequent symptom). Among the 396 patients who declared having symptoms, 152 (39.6%) said that at least one symptom varied over the course of the day, 209 (53.2%) over the course of a week and, together, 241 (60.9%) throughout the day or week. Similarly, 274 (58.1% of the total and 69.2% of the symptomatic patients) reported that their symptoms varied in accordance with the seasons of the year, with worsened symptoms in winter and in summer. The percentage of patients who perceived variability in each of the symptoms studied over the course of a day or week, compared with the total number of patients with that symptom, is presented in Fig. 1. It is observed that chest tightness and dyspnea are the symptoms that are most frequently perceived as variable, and expectoration is that which is most often perceived as constant.
Frequency of Respiratory Symptoms in the Population Analyzed.
| No symptoms | 75 (15.9%) |
| Some symptoms | 396 (84.1%) |
| Frequency of the symptoms | |
| Dyspnea | 226 (47.9%) |
| Cough | 235 (49.8%) |
| Chest tightness | 111 (23.5%) |
| Expectoration | 264 (55.9%) |
| Wheezing | 163 (34.5%) |
| Number of symptoms declared | |
| 0 | 75 (15.9%) |
| 1 | 102 (21.6%) |
| 2 | 85 (18%) |
| 3 | 111 (23.5%) |
| 4 | 56 (11.9%) |
| 5 | 30 (6.4%) |
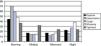
Those patients who declared that one or more of their symptoms varied throughout the day were asked what moment of the day they associated with greater symptom intensity. The results are expressed in Fig. 2. All symptoms were clearly predominant in the morning and even more so for cough and expectoration. Contrarily, chest tightness was more predominant in the morning, but to a lesser degree.
Impact of the Symptoms in Daily Activities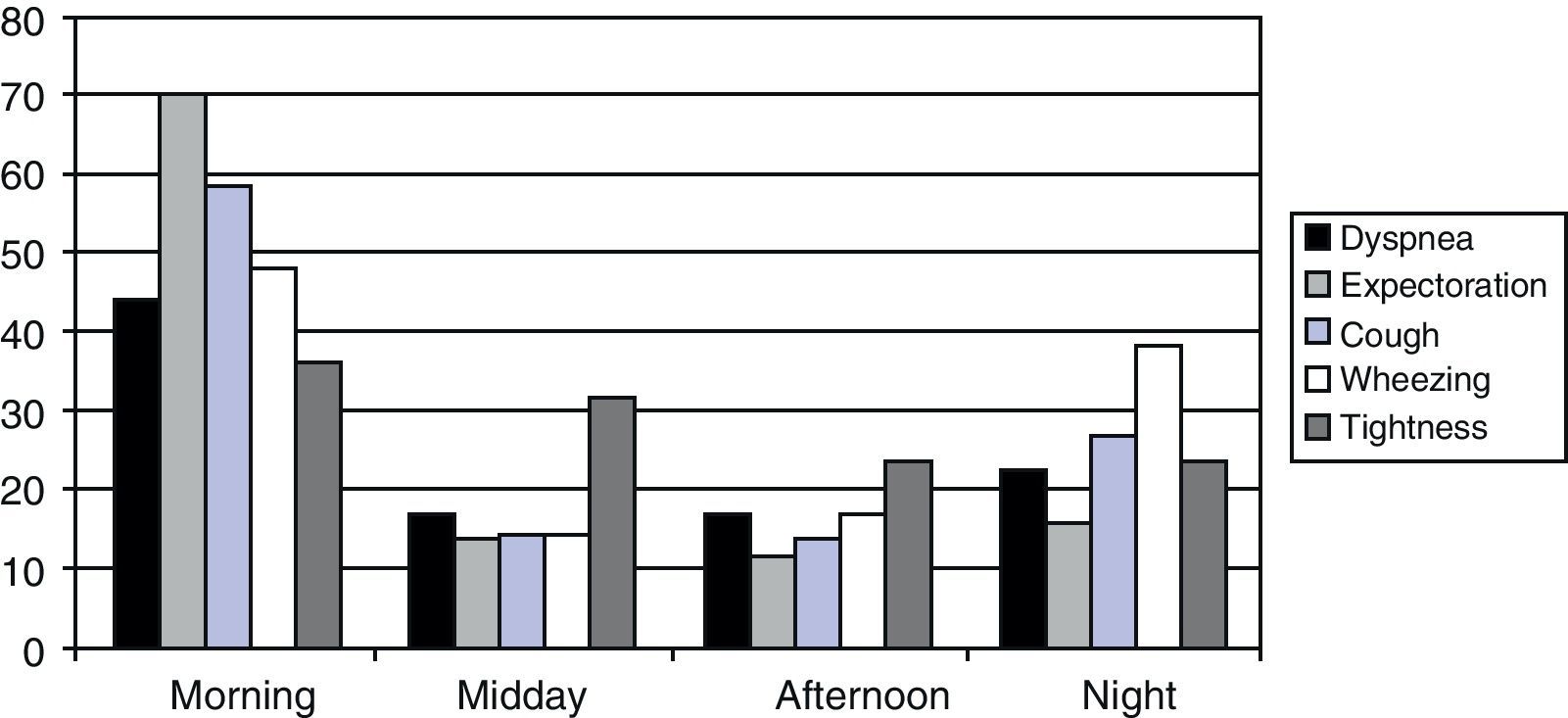
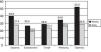
In order to know the level of general activity of the population, the individuals were asked the amount of time that they walked and the amount of time that they spent watching television each day on average during the week prior to the study. 34.3% walked an average of 30–60min and 39% more than 60min daily (Fig. 3A). It is also striking that 55.1% spent more than 3h per day watching television (Fig. 3B). When asked about the impact of the symptoms on morning activities, 26.5% had some type of impediment to get out of bed, 28.8% had difficulties during personal hygiene and 32.8% to get dressed. 19% declared that their respiratory symptoms affected sleep quality.
Discussion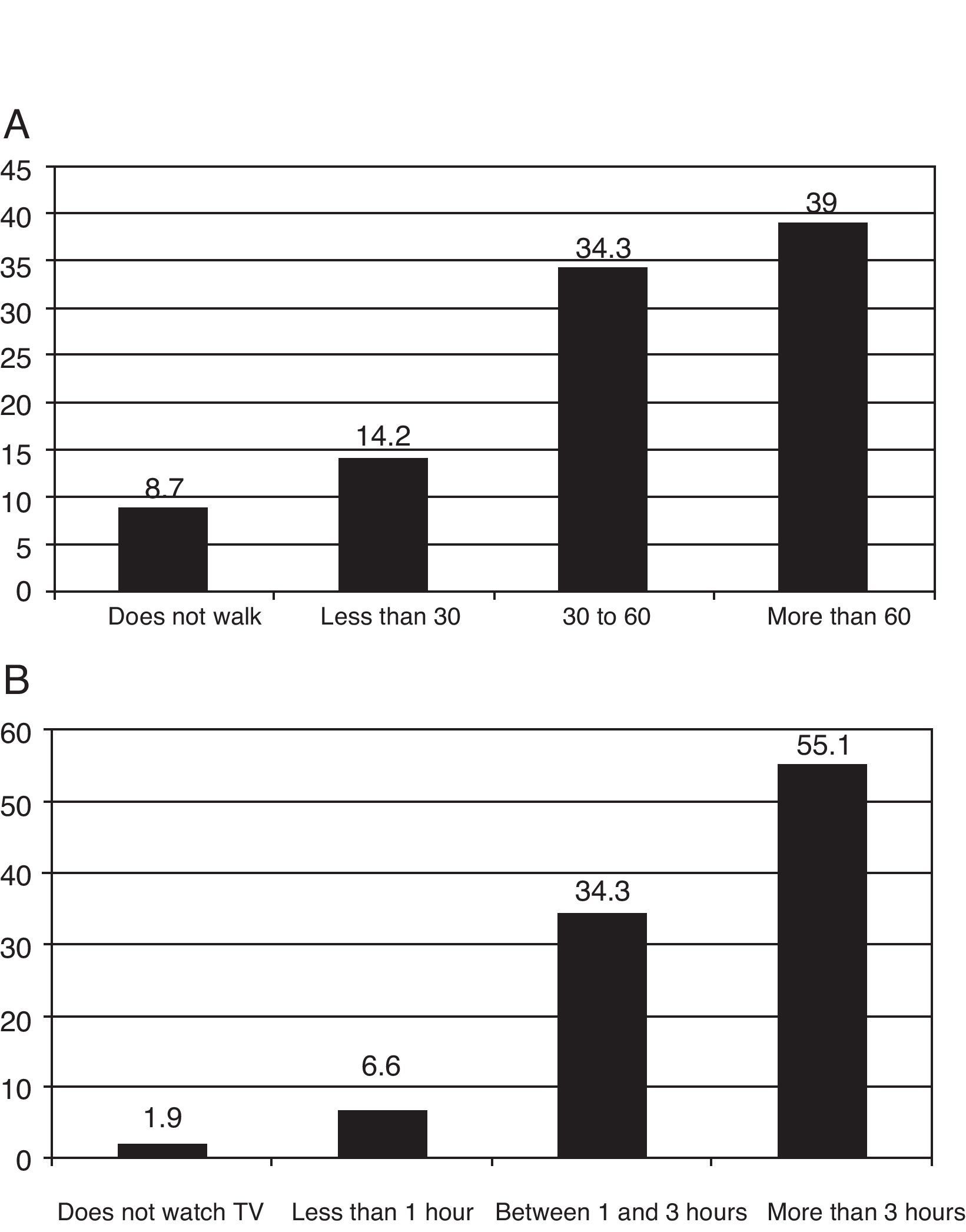
The results of our study have demonstrated that the majority of severe COPD patients perceive significant variability in their respiratory symptoms either during the day or over the course of the week. The mornings are the part of the day in which these symptoms are perceived with greater severity or intensity and when they interfere to a greater degree with daily activities. These results are similar to those found in the European patient population, despite the fact that the Spanish patients presented different demographic and disease expression characteristics.
The Spanish patients included a major percentage of men, with a higher mean age and lower percentage of active smokers. Regarding the symptomatology, in the overall European population 92.5% reported respiratory symptoms compared with 84.1% in Spain. Dyspnea was reported by 72.5% of the total study population,5 but only by 47.9% of Spanish patients. These levels are an example of the differences in the perception of the symptoms between groups of patients with similar disease severity. Previous studies have shown important differences in COPD characteristics6 and exacerbations7 among patients from different countries or geographical areas and climates.9,10 This would explain the detailed analysis of patient subgroups from a specific country or area. On the other hand, the variability in the symptoms was very similar in both populations. In the total population, 62.7% perceived variation in one or more symptoms; 44.7% during the day, and 54.4% during the week,5 compared with 60.9, 39.6 and 53.2%, respectively, for the Spanish patients.
The frequency found of respiratory symptoms in patients with severe COPD may seem low, but it is clearly higher than that found in patients with COPD identified in the EPI-SCAN epidemiological study.11 This is in accordance with the different severity of the disease observed in the patients of both studies and confirms the relationship between the severity of the airflow obstruction and the presence and intensity of the respiratory symptoms. It has also been observed that not only the intensity but also the variability of the symptoms, particularly dyspnea, are greater in more severe patients.5
It is important to note that our population with severe COPD has sedentary habits: 55.1% watch more than 3h of television a day on average, and only 39% walk more than 60min a day. This observation is important because there is a reported relationship between physical activity (specifically, the time spent walking each day) and the risk for hospitalization and death in COPD.12 Furthermore, the increase in time spent walking each day is related with a significant improvement in the quality of life of COPD patients.13
Symptom variability is important because it can lead to the inadequate self-prescription of medication with the intention of alleviating symptoms; it may also be an initial sign that the disease is not under control. Patients who experience greater variability in dyspnea were also those who suffered more frequent exacerbations.5 It would be logical to try to alleviate the symptoms to the fullest extent and reach their lowest possible level of intensity without significant variations. In order to do so, it is important to identify the periods in which the symptoms are more intense in order to adjust the treatment at these moments of greater affectation. In our study, not only winter but in some patients also summer is the season with greatest symptom intensity, which indicates that extreme heat may also be a cause of deterioration in severe COPD. It is interesting to highlight that, for all the symptoms, mornings are, beyond doubt, the time of the day with the greatest symptom intensity and greatest limitation of daily activities. This coincides with the circadian variations in lung function14 and with the fact that mornings are the part of the day that requires greater activity. Another possible cause is the alteration in the quality of sleep, which has been seen in 19% of our population. Previous studies have confirmed that the periods in which the COPD patients feel worse or more incapacitated are the mornings, both in severe as well as in moderate-mild patients.15 For this reason, specific instruments have been designed to enable us to quantify the affectation on quality of life and the activities specifically during this part of the day and to be able to evaluate the impact of therapeutic strategies on the well-being of the patients in the morning.16
The study has some limitations that have been discussed in detail in the group publication.5 Among them are the cross-sectional design and the possible inclusion of patients who are incorrectly diagnosed with COPD and who are, in reality, asthmatics. For the inclusion in the study, pre-bronchodilator spirometry levels were used; this was motivated by the context of the study because an important part of the patients were recruited in primary care, where spirometry is not always available and the bronchodilator test is not usually done.17,18 Nevertheless, we believe that these possible limitations do not invalidate the results obtained.
In short, in an extensive population of Spanish patients with severe COPD, we have observed that respiratory symptoms are perceived as being variable by an important proportion of these individuals. The morning is the time of day when patients are more affected by their symptoms and experience greater interference in daily activities. The reduction or ultimate disappearance of symptom variability should be an objective for COPD treatment.
FundingThe present study has been financed by AstraZeneca.
The organization of the study—including the recruiting of the researchers, patient interviews, collection and handling of the data—was coordinated by Mapi Group, a contract research organization (CRO). The statistical analysis was done by Sami Boussetta (Mapi Group), with funding by AstraZeneca.
Please cite this article as: Espinosa de los Monteros MJ, et al. Variabilidad de los síntomas respiratorios en la EPOC grave. Arch Bronco-neumol. 2011;48:3–7.







