
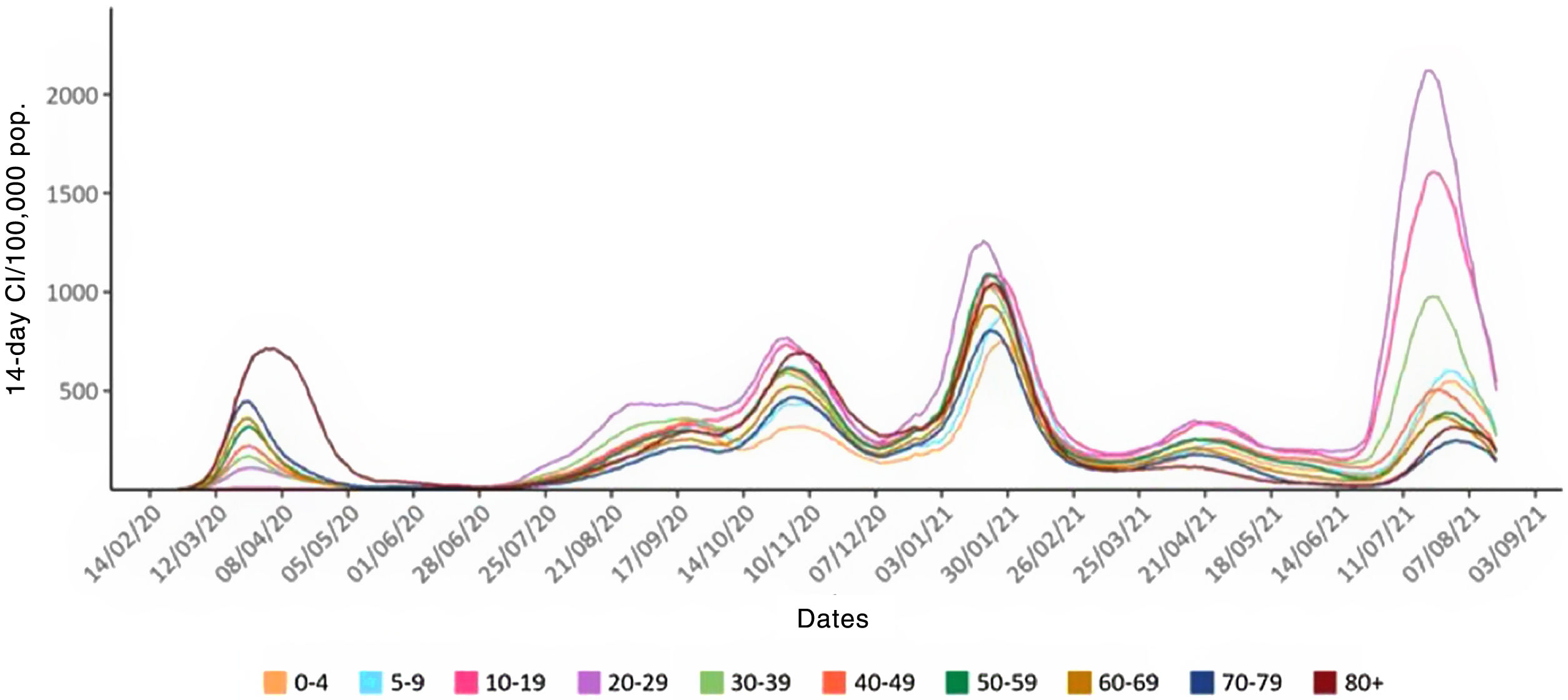
The Beatles, the Olympic rings, the 5 senses, the musical staff. Five is a magic number. We are currently experiencing the fifth wave of the COVID-19 pandemic, which is particularly affecting adolescents and young adults. COVID-19 broke out abruptly in the spring of 2020, bringing high mortality rates, and diagnoses may initially have been underestimated due to the lack of confirmatory tests. The highest infection rates were recorded in the elderly and adults over 50 years of age, and peak mortality rates were recorded in residential centers and nursing homes. The first wave has been followed by successive waves with lower mortality and improved disease diagnosis. A review of incidence over time in the first 4 waves (Fig. 1)1 reveals an interesting pattern. Young people aged 20–29, followed by children aged 10–19, are the age groups with the highest rate of COVID-19 infection since the second wave. This situation was not generally reflected in respiratory medicine departments or in clinics and hospitals, as the proportion of serious complications due to COVID-19 increases exponentially with age, and most of these children and young people had mild and even practically asymptomatic disease.
 by age group in Spain.")
Before this fifth wave, by the end of spring 2021, a vaccination coverage of around 100% had been achieved among the elderly population in Spain. However, since the beginning of summer, young people have been participating in increasingly greater numbers of social and festive activities. This younger population, few of whom are vaccinated (but who have done numerous diagnostic tests), has been the source of another explosion in infections, with 14-day cumulative case incidence figures of more than 2000. Mortality is much lower than in the first wave, but the number of young adults with severe COVID-19 in intermediate respiratory care units and intensive care units in Spanish hospitals is now increasing. The accusing finger must be pointed at the virus, not at the behavior of our young people.
Further research will quantify the effect of factors such as epidemic fatigue, false information, lack of coordination among different administrative bodies, discrepancies in many autonomous communities between public health services and the legislative reality, and the emergence and spread of the new SARS-CoV-2 variants.2,3 In particular, the delta variant, discovered in December 2020 in India and previously known as B.1.617.2, may be a more than likely causative factor of this fifth wave. Delta is a “double mutant” (E484Q and L452R) variant that contains more than a dozen other mutations compared to the original alpha strain detected in Wuhan, China, in December 2019. Delta is already known to have a greater capacity for infection and transmissibility, even in the vaccinated population. Fortunately, the efficacy of the current versions of vaccines against the delta variant seems high.4 The percentage of immunity needed to achieve the long-awaited herd immunity will be much higher than the 70% initially estimated, and given the idiosyncrasy of COVID-19, we may never reach it.5
Our understanding of this new coronavirus is extensive compared to our level of insight just one year ago.6 Treatments that have so far shown significant benefits in clinical outcomes of interest include oxygen therapy and/or ventilatory support, prone positioning even in non-intubated patients,7 dexamethasone, tocilizumab, baricitinib, tofacitinib, and REGEN-COV (a combination of casirivimab and imdevimab).8 Other treatments are still being evaluated. Social distancing, masks, and hand hygiene, old measures all taken in previous pandemics, remain effective but they need to be used conscientiously and persistently.
There are still many more questions than answers, and it is more than likely that we will face a sixth wave.9 In addition to the 4 classic elements (earth, water, fire, and air), a fifth element, such as ether, will likely be needed to confront this fifth wave of pandemic. In short, COVID-19 is a new disease with global distribution that may become endemic. It will remain a challenge but also an opportunity.10,11
In esoteric thought and numerology, 5 is the number of change, movement, and mutation, guiding us to mastery through experimentation. Will this fifth wave and the pandemic in general help achieve better, universal, free healthcare and lead us toward fairer global governance?
All three authors are members of the COVID Medical Commission of the Universidad Autónoma de Madrid. JBS was Senior Consultant of the WHO Health Emergency Program COVID-19 Clinical Management Team, World Health Organization HQ, Geneva, Switzerland, between October 2020 and June 2021.







