

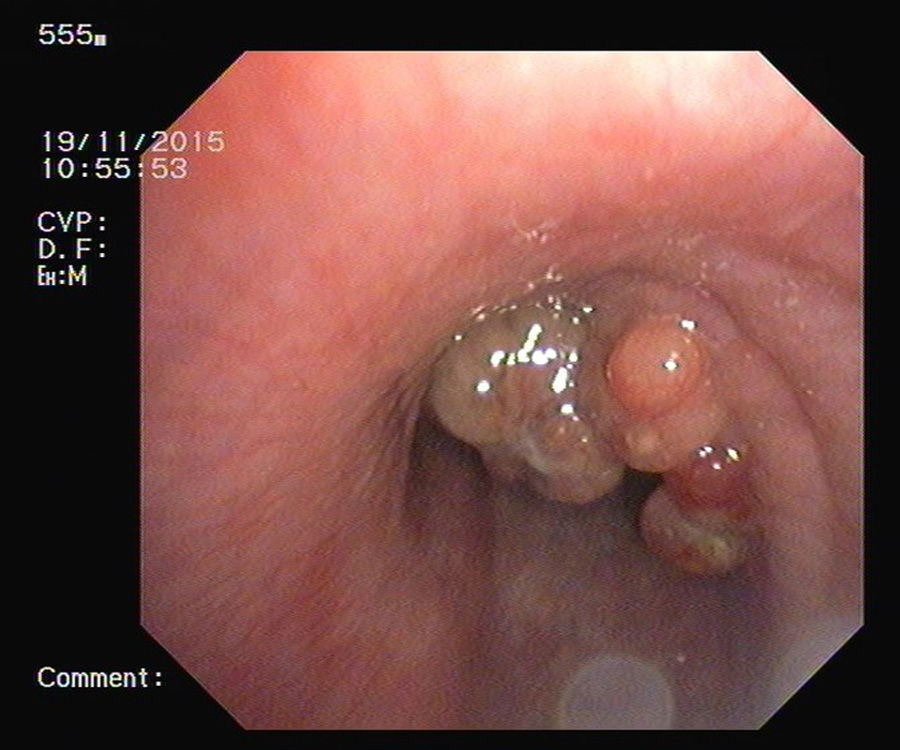
This is an endoscopic image (Fig. 1) from a 40-year-old woman who presented with a 3-month history of cough and progressive dyspnea. On the chest computed tomography (CT), a mass could be seen in the anterior segment of the right upper lobe (RUL), invading the mediastinum and surrounding the tracheal bifurcation, with signs of tracheal invasion of the right primary bronchus and the superior vena cava. Despite fiberoptic bronchoscopic resection of the mammilated lesion that obstructed 50% of the tracheal lumen, no diagnosis could be made until a mediastinal biopsy was performed by video-assisted thoracic surgery (VATS), confirming primary mediastinal non-Hodgkin large B-cell lymphoma. After completing 6 cycles of chemotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine, etoposide and prednisone, complete radiological and metabolic response was observed on PET-CT with 18FDG, and the patient achieved full remission.
Primary mediastinal B-cell lymphoma is a large B-cell lymphoma that arises in the thymus. It mainly affects young adults and accounts for 2%–3% of non-Hodgkin lymphomas in adults. The most common clinical presentation consists of symptoms caused by compression of the mediastinal structures (superior vena cava syndrome, phrenic nerve paralysis, dysphagia, dysphonia or cough). Endobronchial involvement is exceptional.
We thank the Departments of Respiratory Medicine, Thoracic Surgery, Anatomical Pathology and Nuclear Medicine of the Hospital Álvaro Cunquiero, Vigo, Pontevedra, Spain.
Please cite this article as: Valle Feijoo ML, Turcu V, Iglesias Río F, Gutiérrez Mendiguchia C. Obstrucción traqueobronquial secundaria a linfoma mediastínico primario. Arch Bronconeumol. 2017;53:206.







