
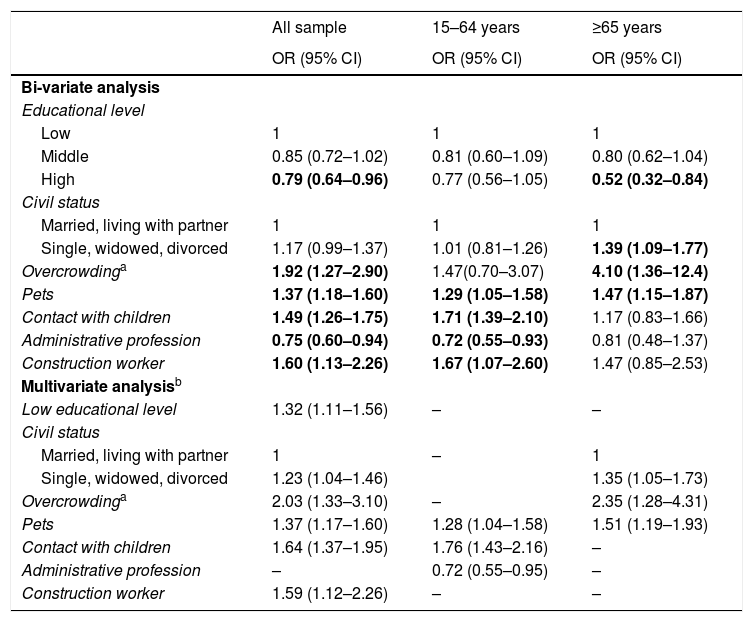
Social determinants of health are the circumstances in which people get born, grow, live, work and age. These circumstances are related with the distribution of money and resources; they determine differences in the exposure to health risk factors and in morbi-mortality.1 Respiratory diseases such as chronic obstructive pulmonary disease have shown a strong social gradient,2 but social determinants of health have not been studied in the case of community acquired pneumonia (CAP). In order to design and implement effective strategies for CAP prevention, knowledge of these risk factors would be useful and of great relevance. We aimed to assess social risk factors for pneumonia in adults and to evaluate if these risk factors are different in younger and older people from data of a large population-based, case-control study conducted in an extensive area of the eastern coast of Spain. Details of the study protocol have been previously reported.3 All cases of CAP confirmed by new radiologic findings of pulmonary infiltrate occurring in the study population during 1 year were recruited. Patients with macro aspiration pneumonia (defined as a pneumonic episode involving loss of consciousness or a witnessed aspiration, and radiographic evidence of an infiltrate in the posterior segments of the upper lobe or the apical or basal segments of the lower lobes),4 active pulmonary tuberculosis, nosocomial pneumonia, and heath care related pneumonia or patients infected by the HIV were excluded. Controls were randomly selected every 3 months from the list of subjects assigned to 64 primary care centres participating in the study. Controls were matched with cases by sex, age (±5 years) and primary care centre. A questionnaire on CAP risk factors was administered by trained physicians or nurses at home. This questionnaire included standardized information related to health habits and lifestyles, clinical conditions or co-morbidities and regular treatments during the last year. Social risk factors considered included education level, civil status, overcrowding (defined as living with more than 10 persons at home), profession, and life conditions such as daily contact with children or pets at home. Odds ratio (OR) was used as a measure of the association between risk factors and the occurrence of CAP and was estimated by conditional logistic regression. Analysis was performed for the overall sample and stratified by age groups (14–64 and ≥65 years). The study protocol was approved by the local Ethical Committee and all participants gave written informed consent before enrolment. A total of 1334 patients with CAP and 1315 controls were recruited with a mean age of 56,1years (SD 20) and 40% were women. Overall, 57.6% of the sample was 14–64 years old and 42.4% was 65 or older. Table 1 presents crude and adjusted effects of different social risk factors for CAP, stratifying by age groups. Low educational level shows an independent effect as a risk factor for CAP in the overall sample analysis, but this variable did not enter in the model when stratifying by age groups. Usual contact with pets is an independent risk factor for CAP in both age groups. In the ≥65 years old group, overcrowding and being single, widowed or divorced are independent risk factors for CAP, while in the 15–64 years old group usual contact with children is an independent risk factor for CAP and work as an administrative is an independent protective factor against CAP.
Social Risk Factors for CAP.
| All sample | 15–64 years | ≥65 years | |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Bi-variate analysis | |||
| Educational level | |||
| Low | 1 | 1 | 1 |
| Middle | 0.85 (0.72–1.02) | 0.81 (0.60–1.09) | 0.80 (0.62–1.04) |
| High | 0.79 (0.64–0.96) | 0.77 (0.56–1.05) | 0.52 (0.32–0.84) |
| Civil status | |||
| Married, living with partner | 1 | 1 | 1 |
| Single, widowed, divorced | 1.17 (0.99–1.37) | 1.01 (0.81–1.26) | 1.39 (1.09–1.77) |
| Overcrowdinga | 1.92 (1.27–2.90) | 1.47(0.70–3.07) | 4.10 (1.36–12.4) |
| Pets | 1.37 (1.18–1.60) | 1.29 (1.05–1.58) | 1.47 (1.15–1.87) |
| Contact with children | 1.49 (1.26–1.75) | 1.71 (1.39–2.10) | 1.17 (0.83–1.66) |
| Administrative profession | 0.75 (0.60–0.94) | 0.72 (0.55–0.93) | 0.81 (0.48–1.37) |
| Construction worker | 1.60 (1.13–2.26) | 1.67 (1.07–2.60) | 1.47 (0.85–2.53) |
| Multivariate analysisb | |||
| Low educational level | 1.32 (1.11–1.56) | – | – |
| Civil status | |||
| Married, living with partner | 1 | – | 1 |
| Single, widowed, divorced | 1.23 (1.04–1.46) | 1.35 (1.05–1.73) | |
| Overcrowdinga | 2.03 (1.33–3.10) | – | 2.35 (1.28–4.31) |
| Pets | 1.37 (1.17–1.60) | 1.28 (1.04–1.58) | 1.51 (1.19–1.93) |
| Contact with children | 1.64 (1.37–1.95) | 1.76 (1.43–2.16) | – |
| Administrative profession | – | 0.72 (0.55–0.95) | – |
| Construction worker | 1.59 (1.12–2.26) | – | – |
Statistical significance was stated at a P value <.05 (the 95% CI does not include 1).
Different social risk factors for pneumonia were identified. In the older group, civil status that might imply to live alone (single, widowed or divorced) was an independent risk factor for pneumonia. This might be explained by a poor self-care and quality of life,5 a bad oral hygiene,6 a low socio-economic status,7 or diminished access to health care services.3 Metersky et al. have described that unmarried elderly men admitted to the hospital with pneumonia have a higher risk of mortality despite having a lower degree of comorbidity.8 Low educational level has also been identified as a risk factor for pneumonia, which agree with previously published studies.9 This effect was especially intense in the older group, although it disappeared in the multivariate analysis probably because of a lack of statistical power. Our study corroborates that living with more than ten persons at home is also a risk factor for pneumonia, especially in old people.10 This can be explained by the direct infection from person to person and the mechanism of transmission of respiratory tract infections (sneezing, saliva, among others), presenting a greater risk in overcrowded homes.11 On the other hand, administrative work was identified as protective factor and construction work as a risk factor for CAP. These findings may be explained by the environmental exposure to dust, smoke, and other known pneumonia risk factors. In the older population these factors were not identified probably because they have an acute or short term effect that disappeared when the exposure is removed. A study limitation was not considering other relevant social factors such as medical insurance and income level. This case-control study shows that social risks factors may play a relevant role in the development of pneumonia and that these factors are somewhat different between young and old adults. As just mentioned, these social factors suggest some mechanisms involved in the genesis of pneumonia, such as the abandonment of personal care and hygiene, the intense personal contact at home or environmental conditions at work, all of them modifiable factors. Further studies are needed to deeply understand the role of social factors in CAP, as well as to assess the effect of social interventionism in the prevention of CAP.12







