



Many diseases in children can manifest as pulmonary cystic lesions. These include congenital malformations, lesions caused by lung infections, collagen disorders, and tumors. The progress and prognosis of these lesions will vary depending on their cause, so the therapeutic approach will be based on our clinical suspicion.
We report 2 clinical cases of young children with solitary pulmonary cysts of very similar radiological appearance, but different causes.
The first patient was a 13-month-old boy who attended the emergency room with a 48-h history of fever and respiratory symptoms. Chest X-ray revealed a solitary cystic lesion in the left lower lobe (Fig. 1A). The examination was completed with a chest computed tomography (Fig. 1B), which confirmed the presence of a thin-walled air cavity in the left lower lobe, measuring 2.9cm×3cm×3.1cm. Our patient's personal history included pneumonia in another site at the age of 6 months, at which time no cystic lesions were observed in the chest X-ray (Fig. 1C). The family also reported that at 12 months of age, the child had had another febrile episode associated with respiratory symptoms, which did not resolve until antibiotics were administered, but no chest X-ray was performed at that time.
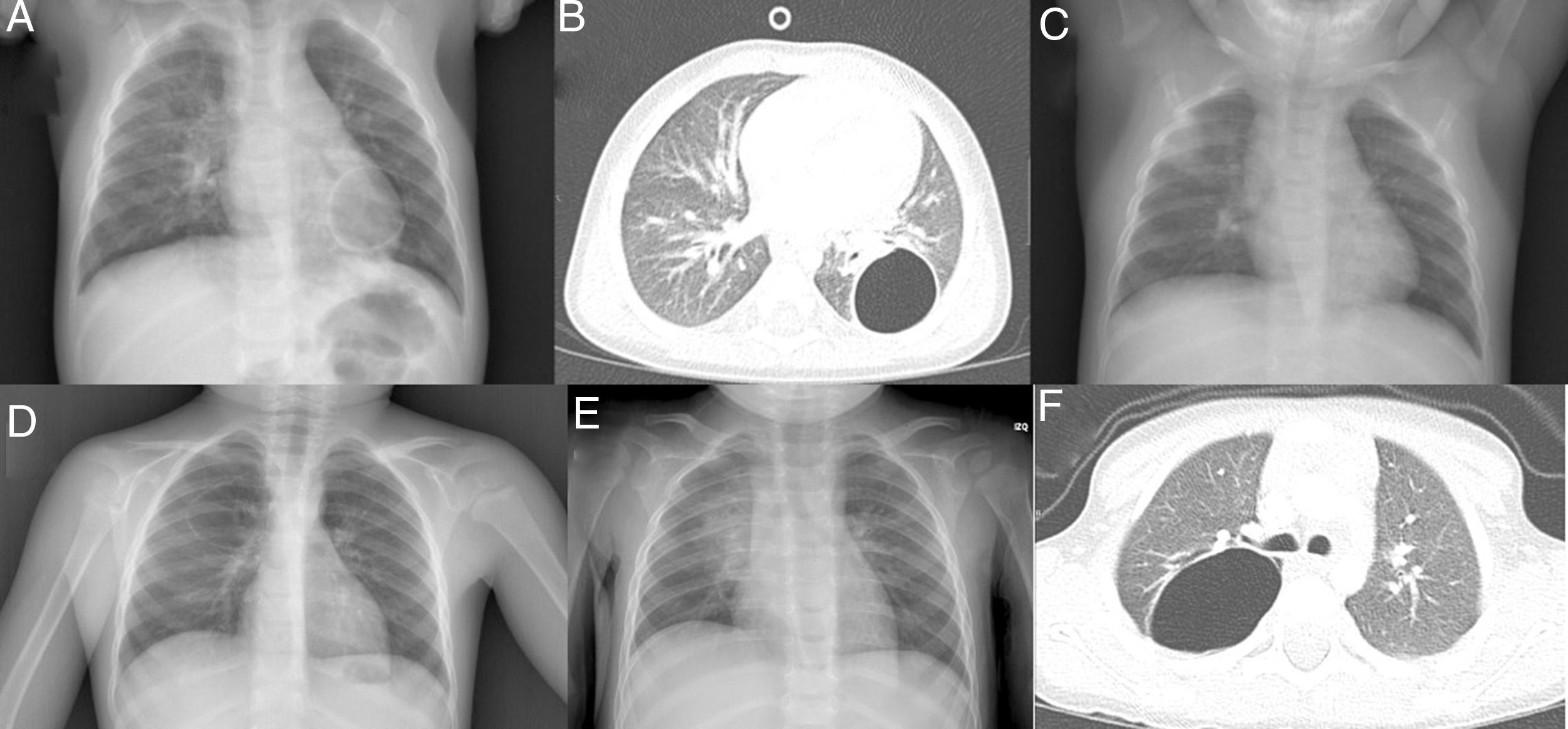
(A) PA chest X-ray: unilocular air cyst in left lung base. (B) Chest CT: thin-walled air cavity in left lower lobe. (C) PA chest X-ray: increased density in right upper lobe of the lung. No cystic lesion is observed. (D) PA chest X-ray: unilocular air cyst in right lung. (E) PA chest X-ray: increased density in right lung. (F) Chest CT: image of thin-walled unilocular cyst containing air, located in the apical segment of the right lower lobe.
Our second patient was a 3-year-old boy in whom a solitary cystic lesion in the right hemithorax was discovered by chance during a chest X-ray (Fig. 1D). The patient was completely asymptomatic from a respiratory point of view. The only remarkable history was an episode of pneumonia in the same site at the age of 11 months (Fig. 1E). Neither follow-up X-ray was performed after that episode, nor were any previous X-rays available. A chest computed tomography was performed (Fig. 1F) to complete the study, confirming the presence of a single thin-walled unilocular air-filled cyst located in the apical segment of the right lower lobe, measuring 4cm×3.5cm×4.5cm, with no other associated lesions.
It is difficult to determine the cause of a solitary cystic lesion purely on the basis of imaging tests. In our patients, the lesions were radiologically very similar, and the subsequent clinical progress of the children was good, with both remaining asymptomatic after diagnosis of the lesion. However, their personal history pointed toward different causes.
In the first case, the previous X-ray in which no cystic lesions were observed allowed us to rule out a congenital malformation, and a pneumatocele due to a respiratory infection was suspected. The patient progressed favorably and the lesion reduced in size in subsequent follow-ups.
It was more difficult to determine the nature of the lesion in the second case, since no imaging test results were available from before the first episode of pneumonia. Our principal suspicion was that it was a congenital pulmonary airway malformation (CPAM) that had been superinfected when the patient was 11 months old, causing the episode of pneumonia. Given the incidental nature of the finding and the lack of symptoms at that time, a wait-and-see approach was taken. After 1 year of follow-up, during which the patient remained asymptomatic and the lesion did not change or reduce in size, we decided to extract it surgically.
Pneumatoceles are thin-walled air cysts usually caused by pneumonia or chest injuries.1 They are typically associated with Staphylococcus aureus infection, but can be produced by other microorganisms. Pneumatoceles generally reduce in size over time, or resolve spontaneously without treatment.1
CPAM (formerly known as cystic adenomatoid malformation) are relatively uncommon congenital malformations that are characterized by replacement of the lung with abnormal, non-functioning, cystic tissue.2 The clinical presentation and progress of CPAM vary widely. More severe disease may cause fetal death or respiratory distress in the early weeks of life, but these abnormalities more often manifest as recurrent respiratory infections during infancy.2,3
In patients with symptomatic CPAM, surgical resection is without question the treatment of choice. However, the optimal management of patients who remain asymptomatic is controversial.2–4 It must be borne in mind that diagnosis before the onset of symptoms is becoming increasingly frequent due to prenatal ultrasounds.
Some authors recommend elective surgery, since the intervention is more complicated and outcomes tend to be worse after the appearance of symptoms. Another argument in favor of surgery is that it can be difficult to distinguish between tumor disease and CPAM on radiology, although there is no clear evidence that the risk of malignant transformation is greater than in the general population.2,4 Moreover, early intervention favors compensatory lung development and avoids exposure to ionizing radiation during follow-up procedures in these patients. Other authors prefer a wait-and-see approach, since the proportion of asymptomatic patients who will end up developing symptoms has not been clearly established, and early intervention may expose healthy individuals to unnecessary surgical risks.2
We report these cases with the aim of highlighting the importance of the patient's clinical and personal history in the diagnosis of solitary pulmonary cysts, since lesions of different etiologies may present indistinguishable radiological images.
Please cite this article as: Nogueira López J, Díaz Munilla L, Viguria Sánchez N, Moreno-Galarraga L. Lesión pulmonar: ¿causa o consecuencia de infección respiratoria? Arch Bronconeumol. 2018;54:295–296.







