

Lymphoepithelioma is an undifferentiated carcinoma characterized by stromal infiltration due to the presence of atypical epithelial cells, associated with a dense benign reactive inflammatory infiltrate, rich in lymphocytes and plasma cells.1 The vast majority of cases occur in the nasopharynx and characteristically in Asian patients, and an etiopathogenic association with Epstein–Barr virus (EBV) has been suggested. When lymphoepithelioma affects other anatomical sites (mostly the parotid salivary glands or the thymus), it is called lymphoepithelioma-like carcinoma.2–7
We report the case of a 66-year-old Caucasian male, ex-smoker of 22 pack-years, with a history of untreated chronic obstructive pulmonary disease GOLD grade 2. As a result of a persistent cough of several weeks’ duration, computed tomography (CT) was performed that showed an irregular consolidation in the middle lobe (ML), multiple bilateral pulmonary nodules, and bilateral hilar and mediastinal lymphadenopathies of significant size, along with moderate pericardial effusion. Blood tests were significant only for raised CYFRA 21.1 (27.5ng/ml) and neuron-specific enolase (50ng/ml). A positron emission tomography (PET) showed increased uptake of 18F-fluorodeoxyglucose both in the ML consolidation and in the mediastinal and hilar lymphadenopathies and lung nodules observed on CT.
Fiberoptic bronchoscopy performed before the PET showed thickened irregular mucosa suggestive of neoplastic infiltration at the entrance of the ML bronchus. The biopsy samples obtained (Fig. 1) confirmed the diagnosis of lymphoepithelioma-like carcinoma of the lung. An assessment was carried out by the ENT department that ruled out the presence of a primary lymphoepithelioma-like carcinoma of the nasopharynx. Three weeks after the first visit, the patient was referred to the medical oncology department with a diagnosis of stage IVA lymphoepithelioma-like carcinoma of the lung (T4N3M1a),8 where he began treatment with carboplatin and pemetrexed. After 2 cycles of chemotherapy, the patient presented both pulmonary and pancreatic disease progression. Finally, a second treatment scheme with carboplatin and gemcitabine began, and he remained clinically stable, with metabolic response according to Response Evaluation Criteria In Solid Tumors (RECIST) criteria.
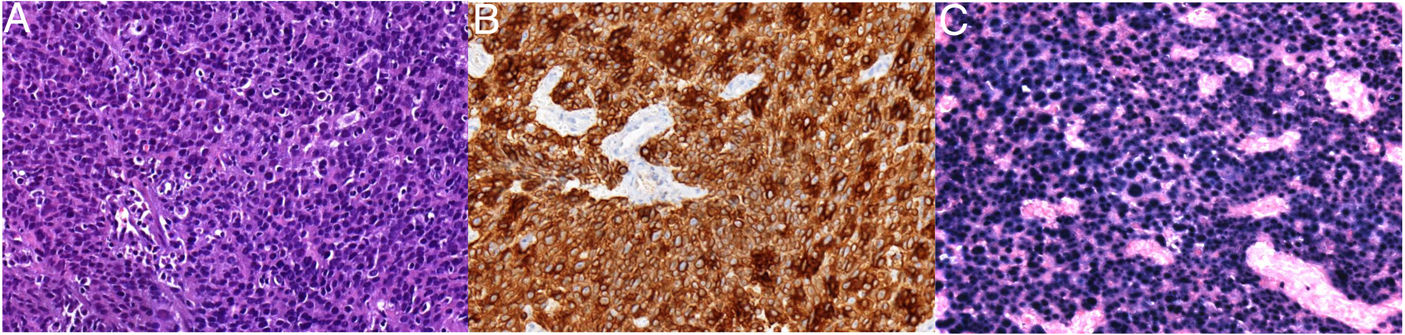
(A) Hematoxylin–eosin staining 100×, showing clear areas of epithelial differentiation with large cytoplasms and eosinophils, and very abundant lymphocytes in the stroma. (B) Immunohistochemical study positive for cytokeratin AE1/AE3. (C) Marked positivity of all atypical epithelial cells for EBER (EBV-encoded small nuclear RNA).
Lymphoepithelioma-like carcinoma of the lung, first described in 1987,9 is one of the most infrequent pulmonary histologic subtypes. Given that the vast majority of cases of lymphoepithelioma-like carcinoma affect the nasopharynx, its presence at this level must be ruled out before pulmonary involvement can be considered to be primary. One of the most important aspects of this type of carcinoma is the potential carcinogenic action of EBV. In fact, the laboratory test used to demonstrate the role of this virus in the genesis of lymphoepithelioma-like carcinoma identifies fractions of non-coding RNA located in the nucleus of cells infected with the virus (Epstein–Barr virus-encoded small RNAs [EBERs]).10 It is believed that EBER particles, first described in 1981, interact with a variety of host proteins to form ribonucleoprotein complexes. Although the specific function of EBERs is still not resolved, it is believed that they could play an important role in the oncogenesis of this tumor. Xie et al. propose that the concentration of EBV DNA in blood might be a useful marker in lymphoepithelioma-like carcinoma of the lung, since patients who present high levels in pre-treatment blood appear to have lower survival rates.11 Most patients with lymphoepithelioma are from East Asia (an area of endemic nasopharyngeal carcinoma) and, although it is more common in non-smokers, it appears to be more associated with smoking in the Caucasian population.10–12
Given that the lymphoepithelioma-like carcinoma of the lung is a rare entity, hardly any prospective studies have evaluated the different therapeutic options. In principle, the treatment strategy is the same as for non-small cell lung cancer (NSCLC), with surgical resection as the therapeutic option of choice. In inoperable cases, cisplatin-based chemotherapy would be the alternative to surgery. Some authors have suggested that it is more sensitive to chemotherapy than NSCLC and propose a neoadjuvant regimen in selected cases.13,14 The role of immunotherapy in this type of tumor is currently unknown.15
In conclusion, lymphoepithelioma-like carcinoma of the lung is a very rare tumor, especially in the Caucasian population. EBV probably plays an important pathogenic role, as demonstrated by the identification of EBERs in tumor cells. Therapeutic management is similar to that of NSCLC.
Please cite this article as: Llabrés de Prada M, Martin-Deleon R, Martinez D, Lucena CM, Agustí C. Linfoepitelioma-like primario pulmonar en paciente no asiático. Arch Bronconeumol. 2019;55:600–601.







