

Most patients recover completely after infection with SARS-CoV-2 and COVID-19, but about 1 in 6 patients develop symptoms that persist beyond the acute phase.1 Long COVID encompasses a number of ill-defined conditions that occur in patients surviving acute COVID-19. There is an urgent need of recognition, research and rehabilitation of patients with long COVID.2 Already a few interventions are recommended for reducing the incidence and severity of long COVID, namely booster vaccinations, early antiviral therapy, and metformin, while other options are being considered.3 The mechanisms involved in long COVID are considered multiple and most likely intertwined; they may change within the same patient, and perhaps with time.4 Similar to other post-infection (i.e.; tuberculosis, HIV, Zika, …) or non-communicable (metabolic syndrome, COPD, …) conditions, where multiple drugs in a fixed combination have been tested successfully,5 combined treatments might be explored in long COVID.
The cardiovascular (CV) polypill consists of a single pill containing three generic components: aspirin, a statin and an angiotensin-converting enzyme (ACE) inhibitor.6 It has become an effective combination for individuals at risk of CV disease,7 as an affordable, safe, easy to comply treatment for the prevention of many CV outcomes.8,9 To the best of our knowledge, beyond the myriad of experimental treatments tested in long COVID,10 none has explored the polypill.
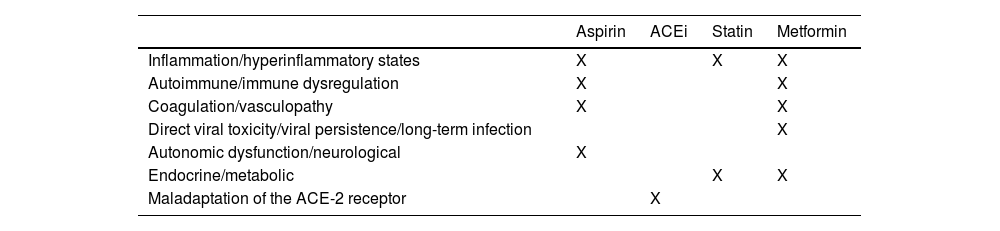
A one-year, pragmatic, randomized, double-blind trial conducted in the primary care setting in adult patients with at least two post-COVID symptoms of moderate or severe intensity (fatigue, brain fog, shortness of breath, body aches, gastrointestinal symptoms, or cardiovascular symptoms) testing a single pill containing aspirin (100mg), ramipril (2.5, 5, or 10mg), and atorvastatin (40mg) plus metformin titrated over 6 days (from 500mg on day 1, 1000mg on days 2–5, then 500mg in the morning and 1000mg in the evening up to day 14 and onwards, versus placebo is envisioned, using as primary and secondary objectives patient-relevant outcomes in long COVID).11 Each of the polypill components might have a benefit in several long COVID mechanisms (Table 1), namely: aspirin with anti-inflammatory, anticlotting, and antiplatelet properties, might also benefit autonomic dysfunction; statins beyond being lipid-lowering, have other beneficial effects on blood vessels and inflammation12; finally, an ACE inhibitor, beyond its antihypertensive properties affects the ACE-2 receptor, which serves as cellular link for SARS-CoV-2.13 Among the above, only one antiplatelet trial has been conducted in severe COVID-19, with inconclusive results.14 There is already available a manufactured polypill, Trinomia®. If only, by adding metformin,15 it would include a new mechanism of action of proven benefit in long COVID.
Potential Beneficial Effects of the Components of a Polypill in Mechanisms of Long COVID: ACE inhibitor, Statin, Aspirin and Metformin.
| Aspirin | ACEi | Statin | Metformin | |
|---|---|---|---|---|
| Inflammation/hyperinflammatory states | X | X | X | |
| Autoimmune/immune dysregulation | X | X | ||
| Coagulation/vasculopathy | X | X | ||
| Direct viral toxicity/viral persistence/long-term infection | X | |||
| Autonomic dysfunction/neurological | X | |||
| Endocrine/metabolic | X | X | ||
| Maladaptation of the ACE-2 receptor | X |
To conclude, long COVID patients often have multiple CV risk factors and comorbidities that provide the rationale for a therapeutic strategy based on a combination of drugs in a single pill against different risk factors. Therefore, many long COVID patients would benefit de novo by reducing their CV risk. However, each component of the polypill might have additional beneficial effects on SARS-CoV-2 and its effects. Overall, there seems to be enough evidence to consider the development and testing of a polypill in long COVID patients.
Conflict of InterestsThe author declares there is no conflict of interests.







