

Placental transmogrification of the lung (PTL) is a rare benign lesion of unknown etiology that occurs more frequently in men. It was first described in 1978 as a lesion that has a topography resembling chorionic villi but no placental biological properties.1,2 Presentation varies from asymptomatic forms to respiratory failure, depending on the presence or absence of underlying disease.1 Lesions have occasionally been described as incidental masses seen on X-ray, but the most common finding is unilateral bullous emphysema and lipomatosis. PTL is often associated with pulmonary fibrochondromatous hamartomas.2
We report the case of a 63-year-old male smoker with an incidental finding of a ground-glass opacity measuring 19mm with a solid component in the left lower lobe. At follow-up, the lesion had not grown, but a cystic, trabeculated component and an increase in the solid component were identified, so a thoracoscopic transsegmental resection of the lesion was performed, giving a diagnosis of PTL with marked lipomatosis. The patient was discharged 48h after surgery. Our case is the first reported case of PTL beginning as a ground glass opacity (Fig. 1).
 Optical microscopy (OM): non-encapsulated lesion composed of papillary structures within hyperaerated cystic spaces and significant presence of adipose tissue with occasional foci of bone metaplasia (arrow) (H&E 2×). (B) OM: a proliferation of capillaries is seen in the interior of papillary structures (arrow) along with abundant mast cells (H&E 10×). (C) CT axial slice: ground glass opacity measuring 19mm in its maximum diameter, located in the left lower lobe. (D) CT sagittal slice: the lesion combines a solid, cystic, and trabeculated component.")
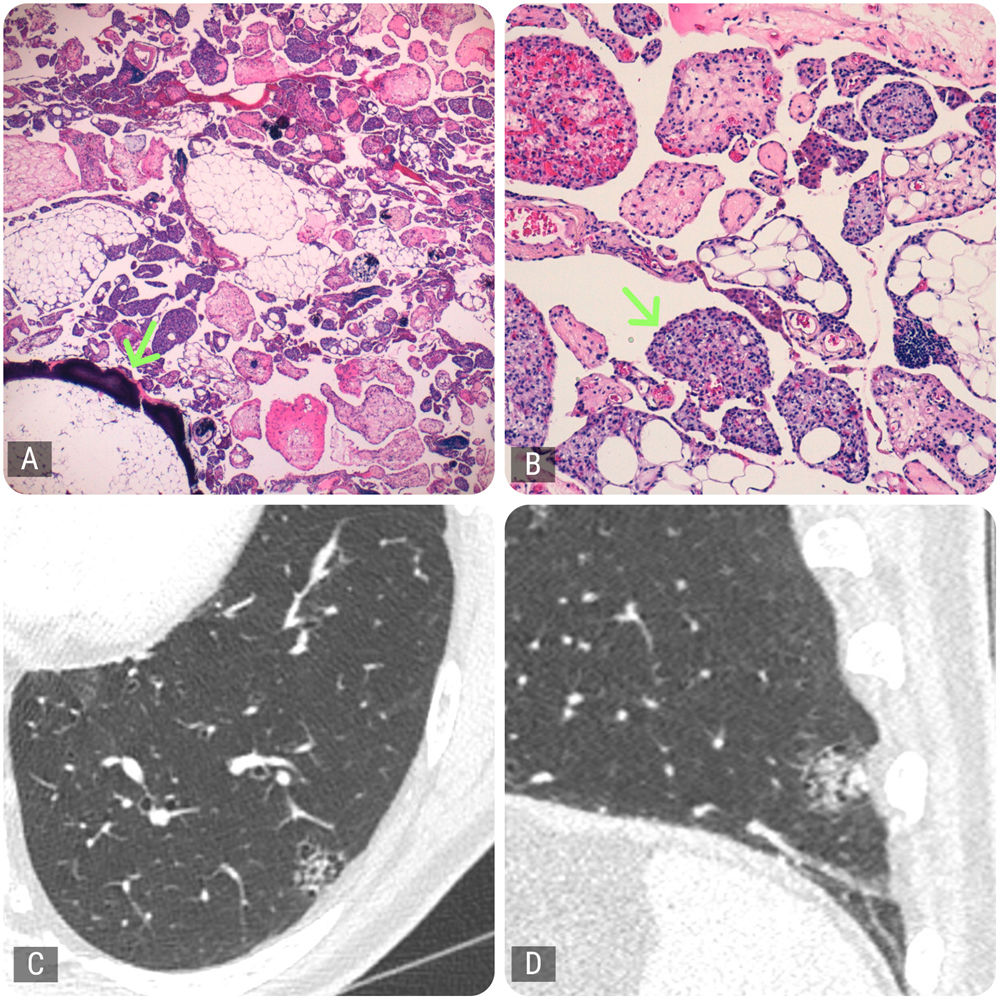
Histology and radiology. (A) Optical microscopy (OM): non-encapsulated lesion composed of papillary structures within hyperaerated cystic spaces and significant presence of adipose tissue with occasional foci of bone metaplasia (arrow) (H&E 2×). (B) OM: a proliferation of capillaries is seen in the interior of papillary structures (arrow) along with abundant mast cells (H&E 10×). (C) CT axial slice: ground glass opacity measuring 19mm in its maximum diameter, located in the left lower lobe. (D) CT sagittal slice: the lesion combines a solid, cystic, and trabeculated component.
We have no conflict of interest or funding to declare and all authors contributed equally to this work.







