
Multidrug resistant tuberculosis (MDR-TB) is defined as TB disease caused by strains of Mycobacterium tuberculosis with resistance to at least isoniazid and rifampicin.1
In any childhood TB diagnosis procedure, major effort must be made to confirm the M tuberculosis strain and the drug susceptibility, as well as facilitating the access to the appropriate treatment.2
The most common clinical form of TB in children is primary TB involving intrathoracic lymph nodes, with a very low bacillary load in their secretions. Despite recent advances, traditional bacteriological tests (bacilloscopy and culture) have a low diagnostic sensitivity (around 30%).3 Therefore, even with negative test results, starting empirical treatment is recommended when faced with clinical and radiological suspicion.1 Moreover, the treatment regimen in children is generally decided upon the results of the drug susceptibility test (DST) performed on the source case (mostly, an adult).4 If the adult is diagnosed with a MDR-TB, the child will be treated as such, and even more so when we know that early initiation of appropriate treatment is essential to ensure good outcomes for both the individual and the community.4
In 2013, the World Health Organization (WHO) endorsed Xpert MTB/RIF® (Xpert; Cepheid, Sunnyvale, CA, USA) for its use in children as an alternative to bacterial culture. It uses a closed, automated system for sample preparation, amplification and real-time polymerase chain reaction (PCR) detection of both M. tuberculosis and rifampicin resistance in only a few minutes.2The Xpert MTB/RIF Ultra cartridge® (Cepheid, Sunnyvale, CA, USA) was developed as the next-generation assay to overcome the suboptimal sensitivity in smear-negative TB patients when using the Xpert MTB/RIF® assay. The sensitivity of Xpert Ultra for detection of Mycobacterium tuberculosis was 64% (95% CI: 48–77%) in gastric aspirate samples and 53% (95% CI: 35–70%) in stool samples. The specificity was 95% in gastric aspirate samples (95% CI: 84–99%) and 98% in stool (CI: 93–99%). The benefit of detecting rifampicin resistance using Xpert Ultra was extrapolated from adult data.2 According to the recent 2021 WHO guidelines, it is strongly recommended as the initial diagnostic test for TB and rifampicin-resistance detection in sputum, gastric aspirate, and other samples rather than smear microscopy/culture and phenotypic drug sensitivity tests in all ages.1,2,4,5
Our aim is to describe a MDR-TB outbreak in a family from a high-income country, Catalonia (Spain), in a low-incidence TB area, where the second-level reference hospital did not have direct access to perform the Xpert method for TB prompt diagnosis.
The primary case was a 5-year-old child with a diagnosis of a probable intrathoracic TB with pulmonary involvement. After twelve days of torpid pneumonia, the chest X-ray (CXR) was compatible with a primary TB with a Ghon complex affecting the right lower lobe and an enlargement of the hiliar lymph nodes. Tuberculin skin test (TST) was positive (13mm), and smear exam was negative. TB treatment with four first-line drugs was started: isoniazid, rifampicin, pyrazinamide and ethambutol.
Through the contact tracing study, a smear positive adult (child's uncle) with bilateral pneumonia and a TST of 20mm was detected, being considered as the source case. Culture for M tuberculosis was performed and he started the same TB regimen treatment as the child.
Other four adults and two children (aged 12 years and 18 months) were living in the same household, all of whom were asymptomatic. The adults were diagnosed with latent tuberculosis infection and treated with a combination of rifampicin and isoniazid. No TB preventive treatment (TPT) was initially prescribed for the 12-year-old girl, with a TST of 0mm and a normal CXR. She was scheduled for a follow-up consultation two months later. The 18-month-old girl had a TST of 12mm and a normal CXR, therefore she started TPT with isoniazid.
Two months later, culture for the primary case was reported as negative, and the antibiogram for the source case came back as resistant to isoniazid and rifampicin, and sensitive to fluoroquinolones and to injectable aminoglycosides.
Regarding the contact cases, a TST conversion (0–25mm) was observed in the asymptomatic 12-year-old girl, and a new CXR showed a consolidation in the left upper lobe with mediastinal widening, highly suggestive of TB. The 18-month-old child, asymptomatic, had mediastinal adenopathies in the thoracic CT scan. In both of them, bacilloscopy and M tuberculosis culture were negative.
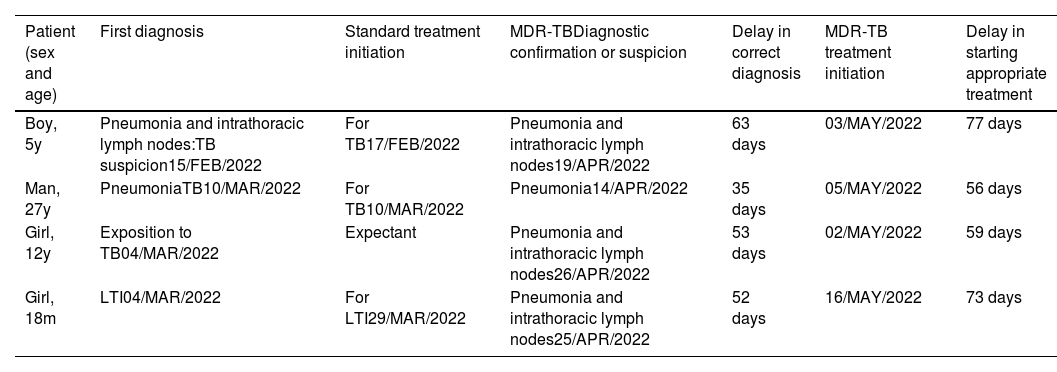
We notified a familial outbreak of MDR-TB affecting one adult and three children, neither of them immunosuppressed or HIV-infected. (Table 1).
Patients with TB disease in the referred outbreak. Delay in diagnosing and starting treatment correctly.
| Patient (sex and age) | First diagnosis | Standard treatment initiation | MDR-TBDiagnostic confirmation or suspicion | Delay in correct diagnosis | MDR-TB treatment initiation | Delay in starting appropriate treatment |
|---|---|---|---|---|---|---|
| Boy, 5y | Pneumonia and intrathoracic lymph nodes:TB suspicion15/FEB/2022 | For TB17/FEB/2022 | Pneumonia and intrathoracic lymph nodes19/APR/2022 | 63 days | 03/MAY/2022 | 77 days |
| Man, 27y | PneumoniaTB10/MAR/2022 | For TB10/MAR/2022 | Pneumonia14/APR/2022 | 35 days | 05/MAY/2022 | 56 days |
| Girl, 12y | Exposition to TB04/MAR/2022 | Expectant | Pneumonia and intrathoracic lymph nodes26/APR/2022 | 53 days | 02/MAY/2022 | 59 days |
| Girl, 18m | LTI04/MAR/2022 | For LTI29/MAR/2022 | Pneumonia and intrathoracic lymph nodes25/APR/2022 | 52 days | 16/MAY/2022 | 73 days |
m: months, y: years, LTI: latent tuberculous infection, TB: tuberculosis.
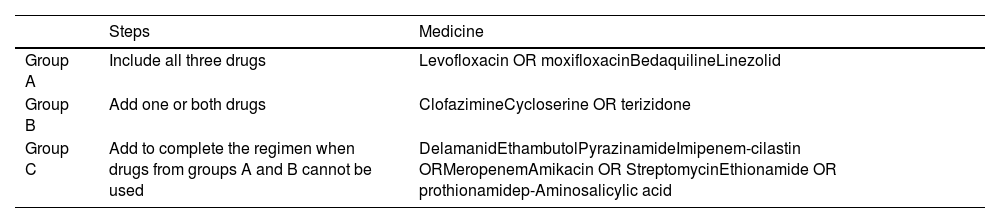
The MDR-TB treatment regimen has to include at least a daily administration of four-five oral second-line drugs5,6 (Table 2).
Grouping and steps to follow for second-line drugs indication, recommended for use in longer MDR-TB regimens.
| Steps | Medicine | |
|---|---|---|
| Group A | Include all three drugs | Levofloxacin OR moxifloxacinBedaquilineLinezolid |
| Group B | Add one or both drugs | ClofazimineCycloserine OR terizidone |
| Group C | Add to complete the regimen when drugs from groups A and B cannot be used | DelamanidEthambutolPyrazinamideImipenem-cilastin ORMeropenemAmikacin OR StreptomycinEthionamide OR prothionamidep-Aminosalicylic acid |
Although since 2022 the WHO recommends the use of bedaquiline in children of all ages with MDR-TB,1,2 in Spain it is only conditionally authorized for patients over 12 years of age.6 Therefore it was not a treatment option in these patients.
Due to this, TB treatment for the 5-year-old boy was changed to a combination of levofloxacin (20mg/kg/day), linezolid (12mg/kg/day), delamanid (50mg/12h), cycloserine (20mg/kg/dia) and clofazimine (5mg/kg/48h).
For the source case, the adult infectologist indicated a change of treatment regime to a combination of moxifloxacin, linezolid, clofazimine and amikacin. The indication of the latter was due to the difficult access to delamanid and bedaquiline.7 Both had received 2 months of useless standard first-line anti-TB treatment. Additionally, the two other asymptomatic children diagnosed with TB recieved the same MDR-TB treatment as the index case, also with a considerable delay (Table 1).
When talking about MDR-TB, some Sub Saharan African countries immediately come to mind, where the pooled prevalence for MDR-TB is 21%,8,9 or some Eastern European countries stand out where a half of the TB cases are MDR-TB.10 In Spain most M tuberculosis strains are sensitive to first-line drugs, being 1.8% of TB cases resistant to rifampicin and 1.2% were MDR-TB in 2020.10
Currently, the WHO recommends rapid molecular tests as the initial test to diagnose pulmonary TB and to simultaneously detect rifampicin resistance.4
In 2020, in Spain, the percentage of notified TB patients diagnosed using WHO-recommended rapid tests (target≥90%) was 31.9%, and first-line DST coverage among them (target=100%) was 46.8%, with a RR/MDR-TB case-detection rate (target=85%) of 10.4%.10
With this letter we want to highlight the ongoing difficulties for prompt TB diagnosis and for obtaining appropriate drugs for MDR-TB treatment in a high-income country with low TB incidence.
In the described outbreak, carrying out a molecular diagnosis test of the source case would have allowed initiation of appropriate treatment much earlier.
In addition, we believe that the use of bedaquiline should not have age restrictions since it has been demonstrated to be safe in all ages.11
To conclude, we underline the need to harmonize our MDR-TB care protocols, with special reference to children and adolescents, following international guidelines; not only applying molecular tests for rapid TB diagnosis and sensitivity studies, but also in improving accessibility to second-line drugs with proven effectiveness and safety, such as bedaquiline.
FundingThere was no funding sources in our research.
Conflict of interestsThe authors declare they have no conflict of interest.







