



Although Castleman's disease is a pathological entity that has been well described in the scientific literature, there are few reported cases in Spain, and they may cause problems in the differential diagnosis. We present the case of a 33-year-old woman referred to our department by Internal Medicine with a diagnosis of a mediastinal mass found on a chest radiograph performed after an accident.
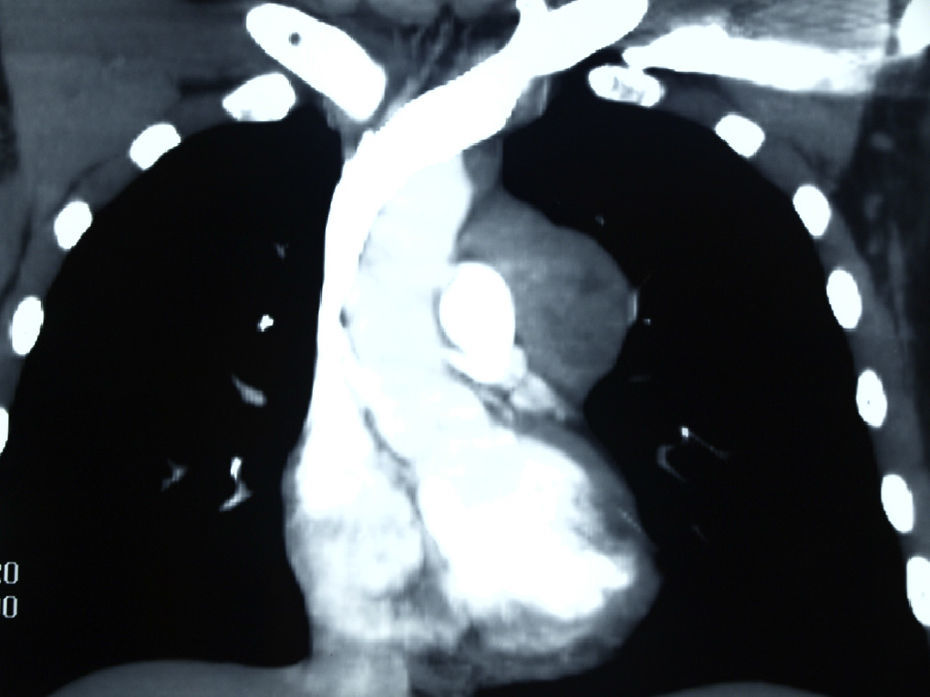
The patient reported an episode of self-limiting haemoptysis one month previously, weight loss that she related with anxiety, occasional retrosternal oppression accompanied by paraesthesia in the left arm and episodes of bronchospasm. Laboratory tests were normal. The chest computed tomography (Fig. 1) revealed a soft tissue mass in the anterior mediastinum, 5cm in diameter, occupying the prevascular space and aortopulmonary window. The lesion first suggested thymoma or lymphoma.
As a surgical approach, we chose a left anterolateral mini-thoracotomy for various reasons: it provides good access to the lesion for biopsy, but at the same time can be easily widened if the lesion is resectable and, moreover, a sub-mammary incision is more cosmetic than an anterior mediastinotomy. A rounded, well-defined mass was found in the mediastinum, which abutted the superior pulmonary vein and artery, pericardium and left upper lobe, but did not infiltrate any of these structures and was completely excised.
The specimen was sent as an intraoperative biopsy and diagnosed as thymoma.
Definitive pathology: 6.16×4.67cm rounded, well-defined tumour. Benign giant lymph node hyperplasia consistent with Castleman's disease, histological subtype hyaline-vascular.
Castleman's disease (also known as angiofollicular lymph node hyperplasia or benign giant lymph node hyperplasia), first described by Benjamin Castleman in 1956,1 is a rare entity characterised by non-tumour proliferation of lymphoid tissue. The cause is unknown, although a subgroup of cases is associated with human herpesvirus-8 (HHV-8).2
It affects both sexes equally and can appear at any age and in any part of the body, although it occurs mainly in the thorax (70%), followed by the neck (15%) and the abdomen-pelvis (15%).
Castleman's disease is classified into 3 histological subtypes: vascular-hyaline, plasma cell type and mixed.3 More recently though, a new classification into 4 variants has been proposed4: vascular-hyaline, plasma cell type, HHV-8-associated and non-specific multicentric Castleman's disease. The vascular-hyaline type is the most common variant (90%). It usually affects young people and is associated with the localised form. The plasma cell type represents 9% of cases, appears in adulthood and is usually characteristic of the generalised or multicentric form.
Clinically it can present in localised or multicentric form. The localised form appears more frequently in the thorax. The mean age is around 35 years and it affects both sexes equally. It usually presents as an asymptomatic, isolated mass, often diagnosed as a casual finding. It occasionally causes symptoms of compression, such as chest or abdominal pain. Peripheral lymphadenopathies are rare and laboratory tests show abnormalities in only 25% of cases. The multicentric form usually appears in older patients, affects more than one area of the body and presents with systemic manifestations: asthenia, weight loss, fever, generalised lymphadenopathies, skin lesions, neuropathy and hepatosplenomegaly. Laboratory tests usually show increased ESR, anaemia and hypergammaglobulinaemia. Unlike the localised form, it is strongly associated with immunosuppression and HHV-8 infection.2 Its clinical evolution is often aggressive and fatal due to the development of infections and neoplasia, such as Kaposi's sarcoma and lymphomas.
The disease is suspected using imaging techniques, but definitive diagnosis requires a biopsy. The differential diagnosis includes other lymph node diseases, particularly lymphomas and tuberculosis, and indeed Bonekamp et al. called it “the great mimic”.5
Treatment in the localised form is surgical resection6; recurrence has not been reported in most series, even with incomplete resection. The multicentric form requires multimodal therapies with radiotherapy, chemotherapy, corticosteroids and monoclonal antibodies.5
Conflict of InterestThe authors do not have any conflicts of interest.
Please cite this article as: Miguélez Vara C, et al. Enfermedad de Castleman mediastínica: presentación de un caso. Arch Bronconeumol. 2013;49:455–6.







